


I informed you thusly: Part 3
Molnupiravir causes transmissible mutations in SARS-CoV-2

Ok, so I told you masks don’t work to prevent respiratory virus infection and transmission, and now the latest Cochrane review has confirmed that they don’t work.
Aaaaand, I told you that neither influenza vaccines nor COVID-19 vaccines prevent infection with, or transmission of, the viruses associated with them, and now Dr Anthony ‘I Am the Science’ Fauci himself has confirmed that neither they, nor any other vaccines for respiratory diseases caused by viruses that replicate predominantly in the respiratory mucosa, prevent infection or transmission.
Let’s try for three for three.
I told you back in May 2022 that Merck’s antiviral drug molnupiravir (sold under the brand name Lagevrio) generated mutated versions of SARS-CoV-2 that were shed in recipients’ nose and throat secretions, and could potentially lead to new, transmissible variants of unknown virulence. Our fearless drug regulator, the Therapeutic Goods Administration (TGA), airily dismissed the significance of this finding on the say-so of an unnamed ‘independent expert’:
“The likelihood of mutations resulting in a more virulent strain of SARS-CoV-2 from treatment with molnupiravir over the long-term has not been assessed. It is less likely, but unproven, that virus mutation induced by molnupiravir will increase virulence of SARS-CoV-2.”
As a result of the TGA’s provisional approval of molnupiravir, over 380 000 prescriptions for this twenty year old drug which has never been used before due to concerns about its mutagenicity, had been issued in Australia by December 2022. Australian health authorities are still heavily pushing its use despite evidence of higher death rates in people treated with molnupiravir compared to placebo, and despite the National Clinical Evidence Taskforce in the UK recommending against it:

And now, an international team of researchers has produced compelling evidence that versions of SARS-CoV-2 with mutations consistent with the pattern induced by molnupiravir are showing up in global sequence databases, and that these viral variants are transmissible.
To make sense of the new paper, which has not yet been peer reviewed but was considered significant enough to garner a write-up in Nature – one of the world’s most prestigious scientific journals – we need to do a quick review of molnupiravir’s mechanism of action.
As explained in The great molnupiravir swindle,
“It works by creating errors in the virus’s genetic code, known as mutagenesis. Each time the virus replicates in the presence of molnupiravir, more and more errors accumulate, eventually building up to an ‘error catastrophe’ that stops the virus from functioning.”
(The authors of the new paper dispute the notion of ‘error catastrophe’, and I’ve included their argument as a footnote for those interested in the finer points of this argument.1)
The mutations produced in the viral genetic code by molnupiravir are not random. Instead, they result in very specific substitutions in the four-letter nucleotide ‘alphabet’ that spells out the viral genetic code.
Briefly, in RNA viruses including SARS-CoV-2, the genetic code is comprised of specific sequences of uracil (U), cytosine (C), adenine (A) and guanine (G). During the ‘reading’ of the genetic code that results in protein formation, A and U always pair with each other, while C and G pair with each other. Each three-nucleotide sequence (known as a ‘codon’) represents an amino acid, and the order in which the nucleotides appear dictates the order in which amino acids are strung together to form a protein. (There’s a good summary of this process here for those who want to delve deeper.)
Molnupiravir results in substitution of adenine for guanine (a G-to-A mutation) and uracil for cytosine (a C-to-U mutation). This ‘mispelling’ of the viral code results in masses of mutant virions, most of which are non-viable – that is, they’re unable to do what viruses do to survive, which is to highjack the host cell’s protein-making apparatus in order to make more copies of themselves. However, some of these mutants are viable, and their signature mutations showed up in samples taken from participants in a clinical trial of molnupiravir. These same signature mutations can also be identified and tracked using the global viral sequencing databases GISAID and INSDC.
And that’s exactly what the international team of researchers who wrote this recent paper did.
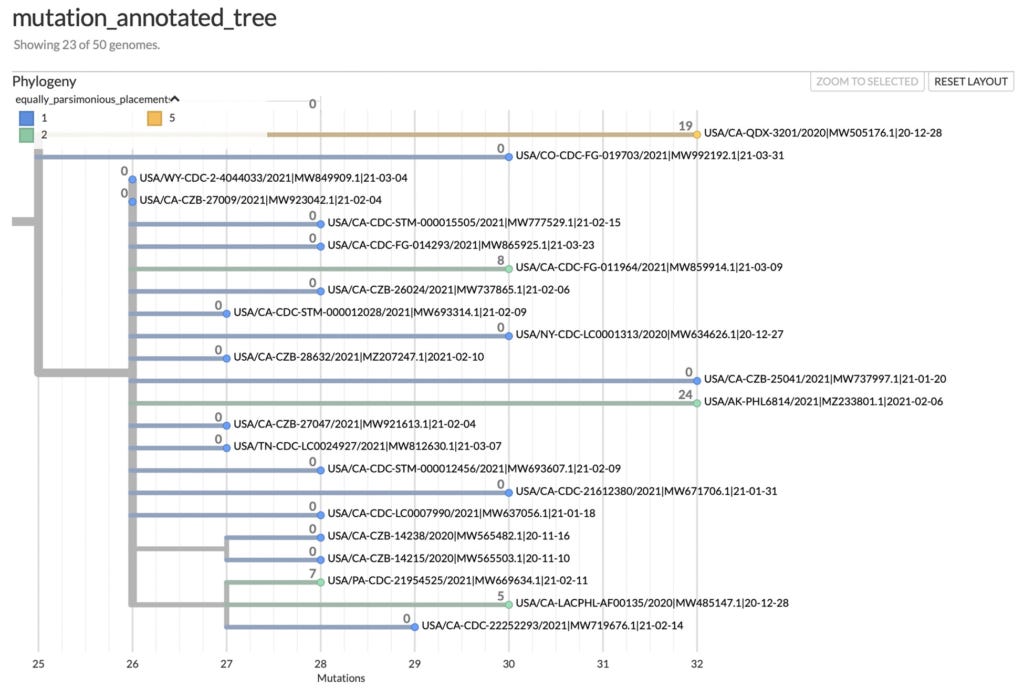
They examined a mutation-annotated phylogenetic tree, which is a method for visually representing the relationships between the genetic sequences of various samples of SARS-CoV-2 that are uploaded to these global databases (see the example below), and identified branches with multiple G-to-A and C-to-U substitutions, consistent with molnupiravir-driven mutation.
Their analysis identified six key facts:
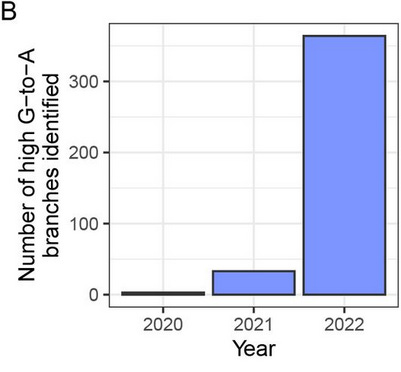
The high G-to-A, and C-to-U branches were almost all sampled in 2022, after molnupiravir entered clinical use. (See Figure 3B below.)
The branches were predominantly sampled from a small number of countries, which could not be explained by differences in the number of uploaded sequences. Specifically, countries which exhibited a high proportion of these branches have been using molnupiravir (these include Australia, Japan, the US and UK) while countries with high levels of total sequencing but a low number of these branches (such as Canada and France) did not approve the use of molnupiravir. (See Table 1 below.)
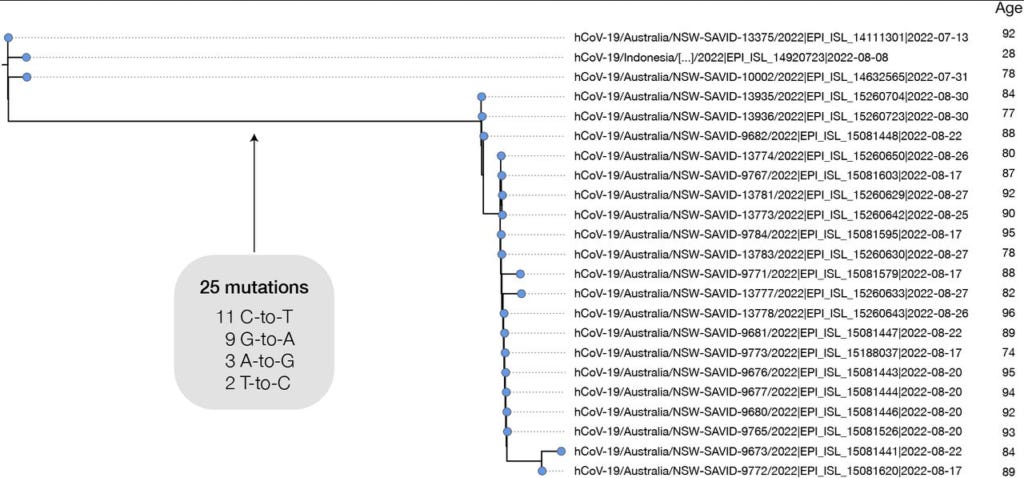
Age metadata provided with uploaded viral sequences shows a significant bias towards patients with older ages for the branches with signature molnupiravir mutations. As the authors point out, “This is consistent with the prioritised use of molnupiravir to treat older individuals, who are at greater risk from severe infection, in these countries. In Australia, molnupiravir was pre-placed in agedcare facilities, and it was recommended that it be considered for all patients aged 70 or older, with or without symptoms.” (See Figure 5 below.)
The mutation rate in the branches with a high G-to-A signature was higher than in branches lacking this signature.
There were multiple examples of such branches giving rise to clusters with a significant number of descendant sequences, suggesting that the sequences derived from multiple individuals who were involved in an outbreak – for example, in a nursing home.
Other sequences showed patterns consistent with “sequences resulting from chronically infected individuals who have been treated with multiple courses of molnupiravir”.

In summary, mutations consistent with molnupiravir’s known mechanism of action, and of the same types that were found in the nasopharyngeal secretions of people who took the drug in a clinical trial, have shown up in global sequencing databases, since molnupiravir began to be prescribed, in the countries which are using it, in the age group for which it is approved, and in patterns which indicate that it is generating transmissible variants with high mutation rates.
When it comes to the implication of their findings, the study authors take a cautious approach. They point out that they have not proved that the use of molnupiravir is driving the mutations that they identified, nor that these mutations are intrinsically more dangerous or transmissible. They call for “public health authorities in countries showing these patterns [to] perform investigations to determine if these sequences or clusters can indeed be directly linked back to use of molnupiravir.”
However, as coauthor Theo Sanderson, a computational biologist at the Francis Crick Institute in London, stressed,
“I would say that our work closes down the possibility that these [molnupiravir-mutated] viruses can never be transmitted.”
COVID drug drives viral mutations — and now some want to halt its use
Rustem Ismagilov, a quantitative bioscientist at the California Institute of Technology in Pasadena who was not involved in the study, stressed that it “underscores the need to quickly measure any risk that molnupiravir poses in terms of sparking new variants, and to weigh them against the drug’s benefits”, adding
“If we are playing Russian roulette, we’d better know our odds.”
COVID drug drives viral mutations — and now some want to halt its use
All I can say is, good luck with that one. I’d lay odds on hell freezing over before any study on the adverse effects of molnupiravir secures funding.
Given molnupiravir’s lack of clinical benefit, the unanswered questions about its capacity to trigger cancer, and these latest findings that point to the strong possibility that it is driving variants with high mutation rates, any sane health authority would drop it like a hot brick. But the TGA continues to insist that it “meet[s] the high safety, efficacy and quality standards required for use in Australia.” One wonders how bad a drug has to be to not meet those standards. (Or perhaps the disqualifying criteria are actual safety and effectiveness, as with hydroxychloroquine and ivermectin.)
Update: 10 March, 2023
Big thanks to Substack reader Garry, who alerted me to the fact that Australian GPs were notified on 5 December 2022 that the National COVID-19 Clinical Evidence Taskforce had updated its listing on molnupiravir and now advised that the drug "should not be routinely used" for COVID due to lack of efficacy in reducing hospitalisations or deaths among higher risk, vaccinated adults with COVID-19. Yet 10 days later, on 15 December 2022, the Commonwealth Department of Health and Aged Care conducted a webinar for primary care providers in which it celebrated the fact that 380 000 prescriptions for molnupiravir had already been issued in Australia, and urged providers to continue writing them (go to 3'6" in the video). TGA has not updated its notice on molnupiravir since 23 September 2022, and still advises its use "for the treatment of adults with COVID-19 who do not require initiation of oxygen due to COVID-19 and who are at increased risk for hospitalisation or death."

What can we ordinary folk do in the face of the complete regulatory capture that is driving unsafe, ineffective and inadequately tested products into the mouths and arms of Australians?
If you have elderly relatives or friends, share this article with them so that they are forewarned and forearmed to ‘just say no’ to any doctor who recommends that they take molnupiravir.
If you are the guardian of a person living in an aged care facility, put the facility on notice that your relative is not to be given molnupiravir.
Print this article out and take it to your local GP or community pharmacist. Ask them if they’re prescribing or dispensing molnupiravir/Lagevrio and if so, do they know that it is ineffective and that the UK’s National Clinical Evidence Taskforce has recommended against its use?
Phone or email your MP and request that they ask a question on notice about the TGA’s continued recommendation of this drug in the face of overwhelming evidence of its lack of safety and efficacy, and its disendorsement by the UK’s National Clinical Evidence Taskforce.
Share this article on social media.
And thank you for slogging through the technical bits in this article, and making it all the way to the end! Together, we are learning our way forward.
For information on my private practice, please visit Empower Total Health. I am a Certified Lifestyle Medicine Practitioner, with an ND, GDCouns, BHSc(Hons) and Fellowship of the Australasian Society of Lifestyle Medicine.
"Molnupiravir’s mode of action is often described using the term “ error catastrophe” – the concept that there is an upper limit on the mutation rate of a virus beyond which it is unable to maintain self-identity (Eigen, 1971). This model has been criticised on its own terms (Summers and Litwin, 2006), but is particularly problematic in the case of molnupiravir treatment. The model assumes a steady-state condition, with the mutation rate fixed at a particular level. The threshold for error catastrophe is the mutation rate at which, according to the model, the starting sequence will ultimately be lost after an infinite time at this steady-state. However molnupiravir treatment does not involve a steady state, but a temporarily elevated mutation rate over a short treatment period. Therefore there isn’t any particular threshold point, or well-defined “ catastrophe” condition. We suggest that the use of this term in the context of mutagenic antiviral drugs is unhelpful. It is enough to think of these drugs as acting through mutagenesis to reduce the number of viable progeny that each virion is able to produce – particularly given that much of the reduction in fitness will be due to “ single-hit” lethal events (Summers and Litwin, 2006)."
The only saving grace (for the general population) that I can see for people being prescribed molnupiravir is that almost all of them are PAST breeding age, and so whatever genetic mutations they may end up with will not be passed on to the next generation!!! :-(
Australia has very much been a 'testing' ground during covid: lockdowns, 'vaccine' mandates, hospital procedures, blocking certain drugs, recommending certain drugs etc. It's disgusting what's been done to people. Just appalling.
Our Aussie Gov is so completely corrupted that even if someone does unequively prove Molnupiravir is dangerous, the TGA will completely and utterly disagree.