


To jab or not to jab? That is the question.

Unsurprisingly, lately my email inbox has been flooded with questions from clients and members of my EmpowerEd program on the COVID-19 injections.
Let me stress at the outset that I do not give advice on medical procedures. However, I do believe in the principle of informed consent which was enshrined in the Nuremburg Code and the Declaration of Helsinki. My role as a health practitioner is to provide information on the risks and benefits of medical procedures, and any alternatives to them, and then leave my clients to make the decisions for themselves based on their personal values, including the weights they place on those risks and benefits.
I’ve previously written five articles on this topic (COVID-19 vaccines: Magic bullets or mirages?, Meet the criminal corporations developing COVID-19 vaccines, Government marketing campaign for COVID-19 vaccines: “dispelling fears” by avoiding the facts, COVID-19 vaccines and the fine art of doublethink and Is the COVID-19 injection roll out a violation of the Nuremburg Code?), and also made a video (WHO’s plan to vaccinate the world), which I strongly recommend that you read and watch. These will provide the full context of this relatively brief summary of the key questions that I believe you should be asking before accepting any COVID-19 injection.
Question 1: What is my risk of developing COVID-19?
Becoming infected with the novel coronavirus SARS-CoV-2 does not mean that you will develop COVID-19. COVID-19 is a disease state, and by definition, a person who does not have symptoms of a particular disease, does not have that disease.
There are no ‘COVID tests’, only tests that measure either the presence of SARS-CoV-2 in your respiratory tract (RT-PCR tests, antigen tests), or your immune system’s response to it (antibody tests).
Most people who receive a positive RT-PCR test result will never go on to develop COVID-19, because in areas with low circulation of the virus, such as Australia, over 90% of positive test results are false positives.
Even if the result is a true positive, for the vast majority of people, infection with SARS-CoV-2 results in either no symptoms at all, or mild common cold-type symptoms that should simply be intelligently managed as per the guidelines in my article Amusing COVID-19 patients to death with fever suppressing drugs: no fever-suppressing drugs, no over-hydration, and restricted food intake (or complete fasting, if there are no contraindications).
If you want to get a more precise indication of your risk of developing COVID-19, you could use Oxford University’s QCovid calculator. I plugged in my personal details and here’s what I got:

Bear in mind that my 1 in 2793 risk of being hospitalised for COVID-19 and 1 in 43478 risk of dying from it are actually significant overestimates, as they are predicated on much higher viral circulation than we have in Australia, which has no meaningful community transmission of SARS-CoV-2.
Question 2: Are there effective treatments for COVID-19?
For those unfortunate enough to develop the inflammatory, thrombotic and vascular features of COVID-19, or for those at high risk of developing them due to pre-existing risk factors such as obesity, diabetes, cardiovascular or kidney disease, there are highly effective protocols both for prophylaxis (prevention of infection) and treatment.
These protocols have been developed by eminent physicians and researchers in the world, including Dr Peter McCullough, Dr Pierre Kory and Dr Tess Lawrie.
Dr McCullough, an esteemed cardiologist, testified before the Texas State Senate Health and Human Service Committee in March 2021 that 85% of hospitalisations and deaths could have been prevented if early at-home treatment protocols for COVID-19 had been implemented.
It is quite literally a crime against humanity that these cheap, safe and effective treatments have not only not been promoted by health officials, but have been actively suppressed by them, with the enthusiastic complicity of the corporate media, foundation-funded media, Big Tech-controlled social media and Australia’s national broadcaster, the ABC.
Fortunately, you and your family members don’t need to live in fear of COVID-19, or suffer or die prematurely, just because certain people and organisations have chosen to keep you ignorant. Thanks to the Internet, you can learn more about these prophylactic and treatment protocols, and read the studies that support them, here, here, here and here.
Question 3: Are the injections effective at preventing COVID-19?
The much-vaunted efficacy of the COVID-19 injections that have been granted provisional approval in Australia, Emergency Use Authorisation in the US, and conditional marketing authorisation in the EU, is largely a mirage.
None of the Phase 3 clinical trials which were used to gain approval/authorisation for each of these products was set up to ascertain whether they prevent severe COVID-19 or death:

To ‘qualify’ for a diagnosis of COVID-19, participants in the clinical trials only had to develop mild symptoms, such as a cough, along with a positive RT-PCR test which, as mentioned above, has a high risk of delivering false positive results. This is not what most people think of when they hear these products touted as “highly effective at preventing COVID-19”!
The phase 3 clinical trials for the COVID-19 injections currently available in Australia will not be completed until February 2023 in the case of the Oxford-AstraZeneca product, and May 2023 in the case of the Pfizer-BioNTech product.
Unfortunately, participants in the Pfizer clinical trial who received the placebo (inactive) injection have now been offered the active treatment, rendering the trial worthless for determining its true efficacy in preventing severe illness, hospitalisation and death.
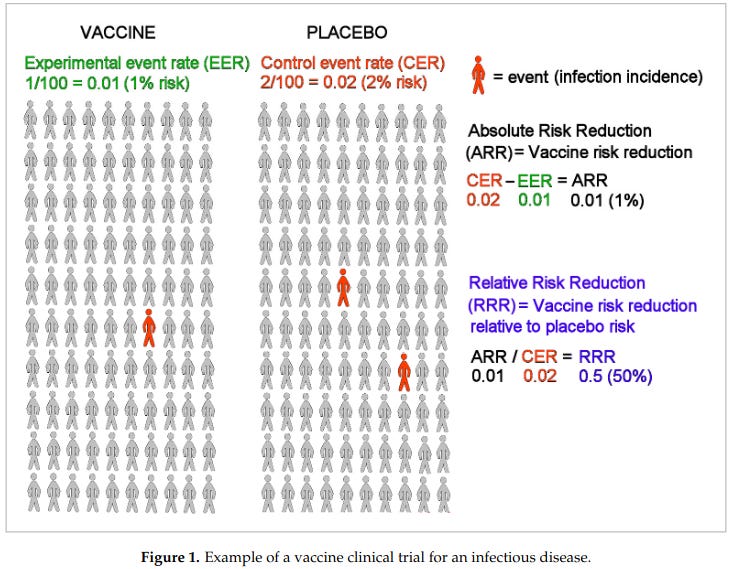
Furthermore, the real-world reduction in risk that these products offer is distinctly unimpressive. The 95% efficacy rate for the Pfizer product that has been plastered all over the press, for example, is a relative risk reduction.
However, the more meaningful measures for an individual weighing up whether to take the jab or not, are the absolute risk reduction (ARR) and the number needed to vaccinate (NNV). The NNV is the number of people who would need to receive the injection to prevent one of them from contracting the disease. ARR is best explained by an illustration of the difference between relative and absolute risks:
Now, here’s the NNV for currently available COVID-19 injections:
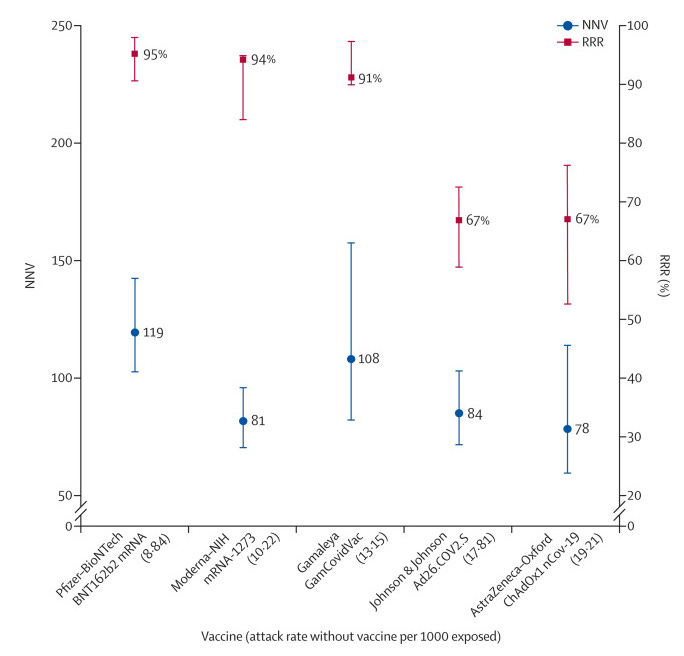
So 119 people would need to receive the Pfizer jab and 78 would have to receive the AstraZeneca jab to prevent COVID-19 of any severity, including minor cold-type symptoms. And that means, of course, that the remaining 118 or 77 people derive no benefit from the injection, but are at risk for all its adverse effects – known and unknown).
And here are the absolute risk reductions:
Oxford-AstraZeneca: 1.3%
Pfizer–BioNTech: 0.84%
Moderna: 1.2%
Johnson & Johnson: 1.2%
Gamaleya: 0.93%
Read those numbers again. Taking these shots will reduce your risk of developing COVID-19 of any severity, including minor cold-type symptoms, by around 1% – and that’s only if you live in an area where the virus is circulating in the community, which it is not in Australia. Impressed? I’m not.
Question 4: Are the injections effective at preventing me from infecting others with SARS-CoV-2?
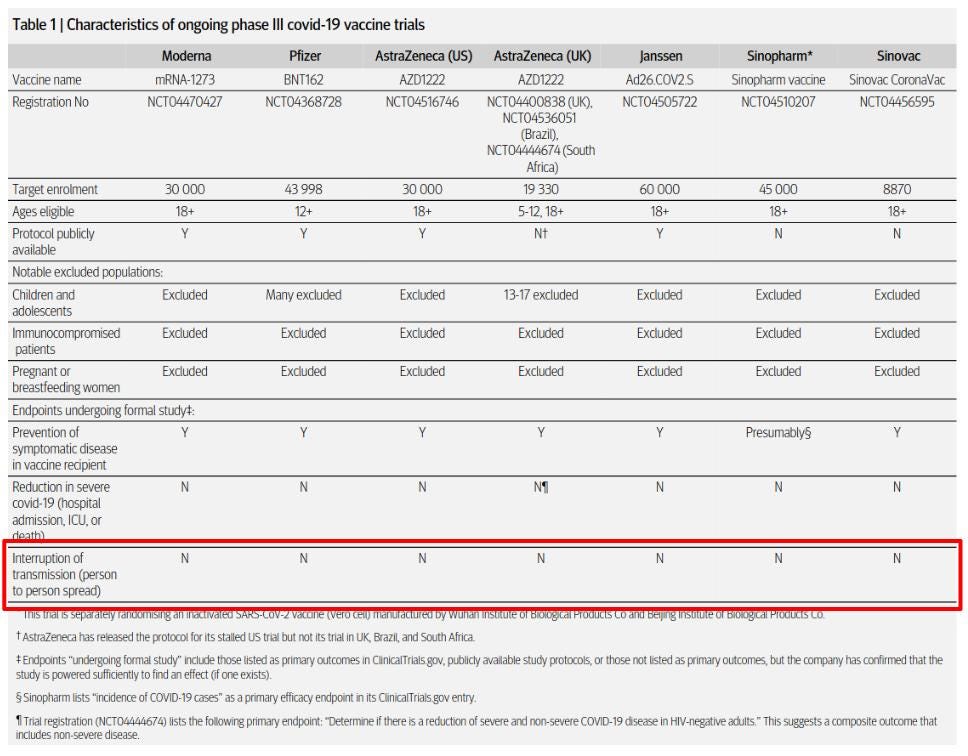
Without data from a properly-conducted clinical trial, it is impossible to determine whether the jabs prevent recipients from infecting others. Certainly, the companies marketing these products have been at pains to point out that they don’t know.
Question 5: Are the injections safe?
An extraordinary number of adverse events and deaths occurring in close proximity to receipt of COVID-19 jabs have been reported to US and European vaccine adverse event surveillance systems. Even more worryingly, these systems are known to capture only a small percentage of actual adverse events.
For example, a study conducted in 2010 by Harvard Pilgrim Health Care, Inc, a large not-for-profit managed care provider, found that “fewer than 1% of vaccine adverse events are reported” to VAERS, the US Vaccine Adverse Even Reporting System.
Here’s a snapshot of VAERS data on COVID-19 injections, current as of the day of writing of this article:

Aside from the severe allergic reactions that occur very soon after injection, none of these adverse events can be definitely stated to be caused by the shots as opposed to coincidentally related to receipt of them.
However, the extraordinarily high number of adverse events, and the fact that 23% of deaths have occurred within 24 hours of injection and 39% of deaths occurred in people who fell ill within 48 hours injection, are certainly safety signals that should be thoroughly investigated, and not brushed under the rug as is currently the case.
In Australia, the Therapeutic Good Administration (TGA) only publishes adverse event reports for medicines and vaccines in the public Database of Adverse Event Notifications 90 days after they are received, which means that adverse event reports for the AstraZeneca shot won’t be available until mid-June.
Question 6: Can I obtain informed consent from my doctor?
According to the Australian Health Practitioner Registration Agency (Ahpra), “practitioners must be careful not to discourage their patient or client from seeking vaccination” regardless of their own vaccination status or views on the subject.
Any practitioner who departs from the script by expressing doubt or concern about the jabs, either during a consultation or on their social media accounts, is liable to be accused by Ahpra of “seeking to actively undermine the national immunisation campaign” and subjected to disciplinary action, including deregistration.
I personally know of several general practitioners who are gravely concerned about the safety of the COVID-19 injections, but dare not speak out for fear of being deregistered and losing their livelihood.
As a health care consumer, if you are not concerned by the fact that the government is inserting itself between you and your doctor, preventing you from having a full and frank discussion with him or her about whether the benefits of receiving a COVID-19 injection outweigh the risks in your particular case, I simply don’t know what to say to you; you’re clearly a completely lost cause with no comprehension whatsoever of the importance of the doctor-patient relationship.
Question 7: Why is the government so fixated on me getting a COVID-19 injection?
Ahpra actually has the hide to warn registered health practitioners that
“It is an offence under the National Law to advertise a regulated health service (including via social media) in a way that is false, misleading or deceptive. Advertising that includes false, misleading or deceptive claims about COVID-19, including anti-vaccination material, may result in prosecution by Ahpra.”
Registered health practitioners and students and COVID-19 vaccination
Yet the same agency is encouraging practitioners to get on board with the government’s demonstrably false and misleading statements about the safety and efficacy of these experimental injections.
TGA has waived its usual prohibition on the advertising or endorsement of medical products to the public in the case of COVID-19 injections, to which it has only granted provisional (not full) registration.
TGA permits doctors and businesses to promote COVID-19 shots and provide “valuable consideration” in the form of discounts, vouchers and special offers, to anyone who accepts a shot. Here are some examples of the kinds of promotional activities that TGA has greenlighted:
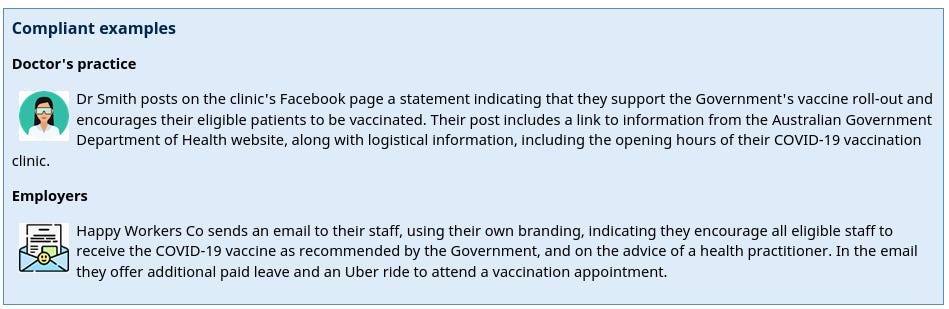
Or perhaps you’d be persuaded to take this experimental product if you were offered a free joint of marijuana, entry in a million dollar lottery, a shot at winning a free college scholarship, free beer, free donuts, or a gift card. I kid you not. These are all real instances of incentives for getting jabbed with an experimental product that has not yet completed phase 3 clinical trials.
If you’re not wondering why you’re being pushed so relentlessly to accept an experimental product with provisional approval, that has marginal efficacy, has been associated with a slew of adverse events, and has an unknown long-term safety profile, to try to prevent an infection that most people suffer either no or mild symptoms of, and that has an infection fatality rate in the same ballpark as influenza, I don’t know how to help you.
But if you are wondering exactly that, congratulations – you clearly have a functioning brain. Keep using it, and keep asking questions. Your health, and even your life, may depend on it.
Awesome work
I don't know how I stumbled on your blog, but you are so funny. My first issue with your articles is that you outrightly show your own bias by calling the vaccine, 'injection'. Secondly, you go on this whole argument that the risk of getting COVID-19 is low. I would like to inform the people who may or may not read this horribly bias take of the coronavirus vaccine. The point in getting vaccinated is for public health. It is not individual health, but it is for protecting the people who are unable to be vaccinated due to auto-immune disorders or other disorders that impact their immune system. To obtain herd immunity, healthy individuals need to be vaccinated by about 90% of the population. So your take that its not worth getting the vaccine, is not only irresponsible, but incredibly misinformed. As a microbiologist, the vaccine reduces the replication of the virus within the body, therefore reducing infectivity and the possibility of variation between strains. So while yes, you may be asymptomatic/mildly sick if you contract covid, vaccination will reduce its ability to replicate in your body and thus infect other people. Just because you say vocab words, does not mean you actually know what the hell you are talking about. Leave science for the scientists. Please and thank you. Remember public health, not individual health. IT IS NOT ABOUT YOU. It is about protecting those in your community (i.e children, and the chronically ill) #getvaxxed :)