


Why Australia's COVID-19 exit plan can't succeed
Part 1

There’s a well-known adage that Australian politicians and public health ‘experts’ would do well to have tattooed on the backs of their hands, so they could remind themselves every day: “When you’re in a hole, stop digging.”
However, despite more evidence surfacing every day that Australia’s COVID-19 policy – which completely contradicts our evidence-based pandemic preparedness plan – is already doing far more harm than good and is doomed to abject failure, our fearless leaders just keep digging.
Both Prime Minister Scott Morrison and NSW Premier Gladys Berejiklian have tied uptake of experimental COVID-19 injections to ending the ongoing nightmare that millions of Australians are suffering through.
Berejiklian, in effect, threatened that if 50% of Sydneysiders don’t roll up their sleeves by August 28, they will remain under house arrest.
Morrison has openly stated that his government intends to implement medical apartheid, offering special ‘privileges’ (which, in the pre-COVID era, we called ‘basic human rights‘) to those who accept an injection while denying them to those who decline.
The Prime Minister told reporters:
“So if you get vaccinated, there will be special rules that apply to you. Why? Because if you’re vaccinated, you present less of a public health risk. You are less likely to get the virus. You are less likely to transmit it.”
‘Special rules’: Vaccinated Australians to avoid lockdown restrictions once 70% target hit
Not only are the divisive and coercive policies embraced by Morrison and Berejiklian morally reprehensible, they are utterly without scientific merit.
Evidence is rapidly accumulating in countries that have already rolled out these experimental injections to large swathes of their populations, that these rushed-to-market products are
Abjectly failing to prevent infection with and transmission of SARS-CoV-2;
Incapable of achieving herd immunity;
More than likely responsible for the development of new variants of SARS-CoV-2 that are resistant to any ‘immunity’ they may confer; and
Possibly sowing the seeds for a devastating wave of serious illness thanks to vaccine-induced escape mutants and antibody-dependent enhancement.
In this week’s post, I’ll lay out the evidence for the first two claims.
COVID-19 ‘cases’ are rising in highly-‘vaccinated’ populations
Let’s look at a few of the poster child nations and states which have achieved high ‘vaccination’ rates against COVID-19.
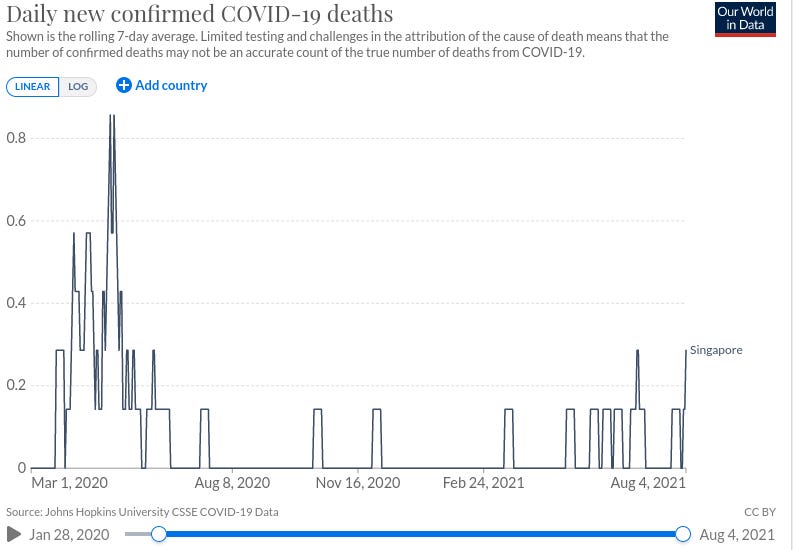
1. Singapore
Singapore has administered COVID-19 injections to 75% of its entire population, with 50% considered ‘fully vaccinated’.
Yet as the number of injections administered rose, it recently experienced a spike in cases, and deaths:
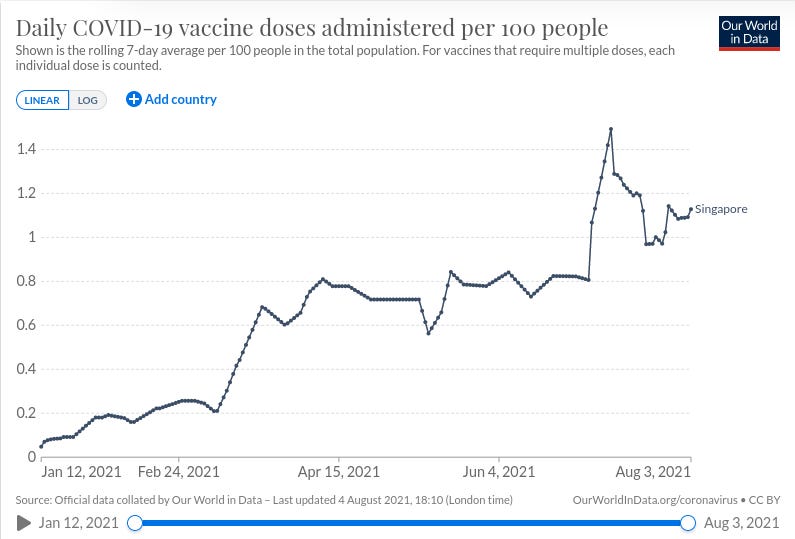
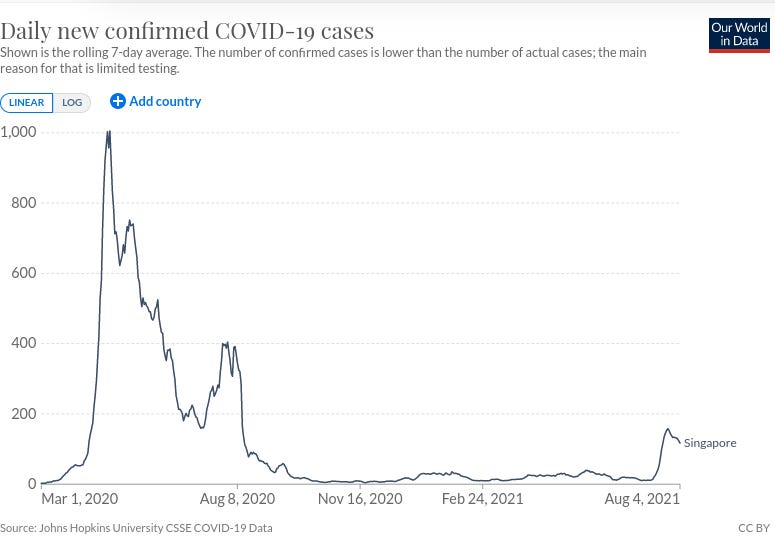
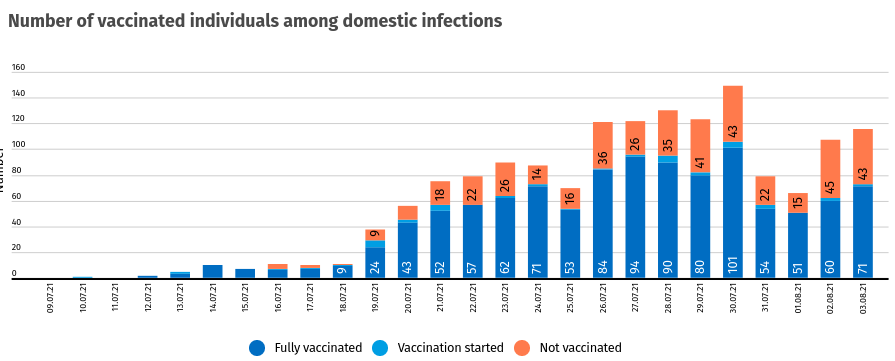
Furthermore, 74% of SARS-CoV-2 infections reported in July 2021 were in people who had already received their jabs (44% in fully vaccinated people, and 30% in partially vaccinated).
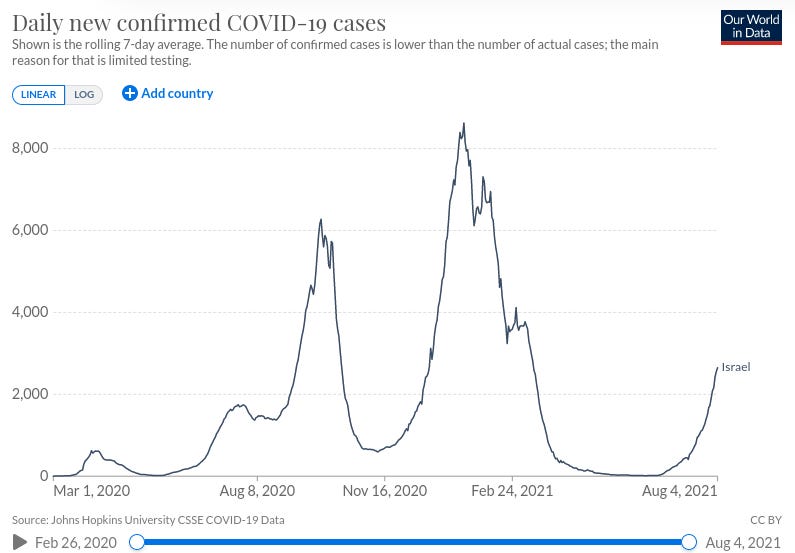
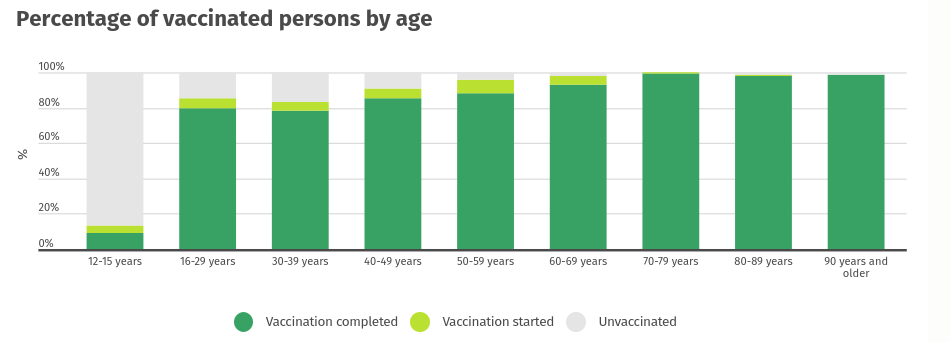
2. Israel
Over 62% of Israel’s population is ‘fully vaccinated’, yet both cases and deaths are rising rapidly:
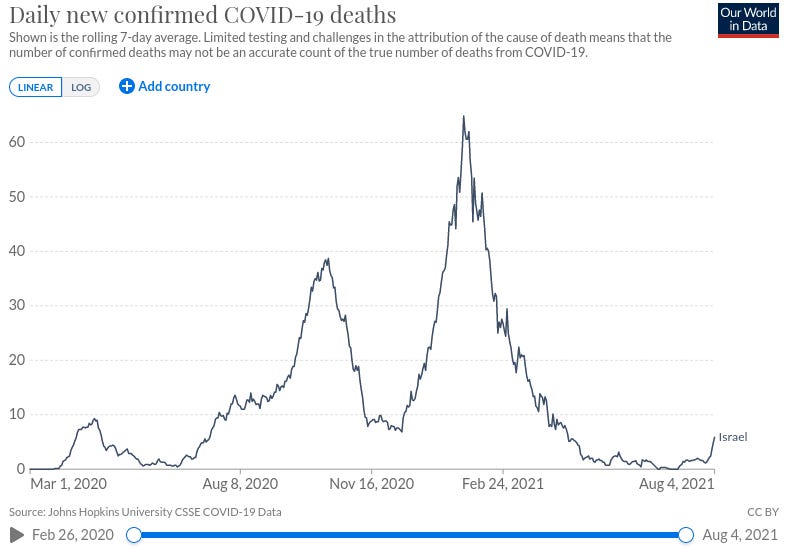
Moreover, according to Israeli health ministry data reported by the media on 19 January 2021, 6.6% of people tested positive after receiving a vaccine dose, at a time when the rate of positive cases in the general population was below 5%.
More recent data indicate that the majority of severe cases, hospitalisations and deaths are occurring in fully-‘vaccinated’ individuals (red is unvaccinated, yellow refers to partially ‘vaccinated’ and green fully ‘vaccinated’):




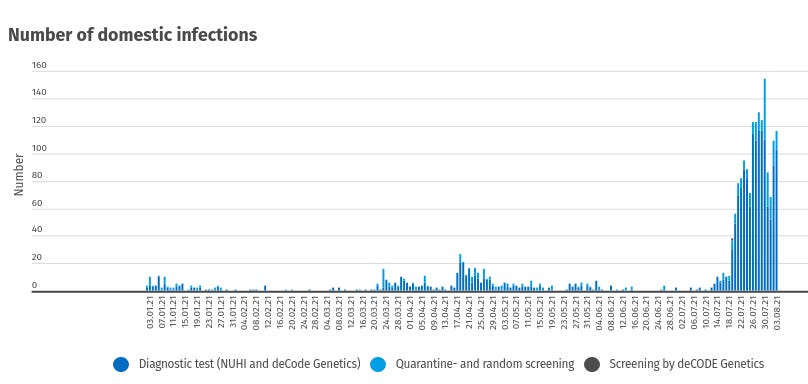
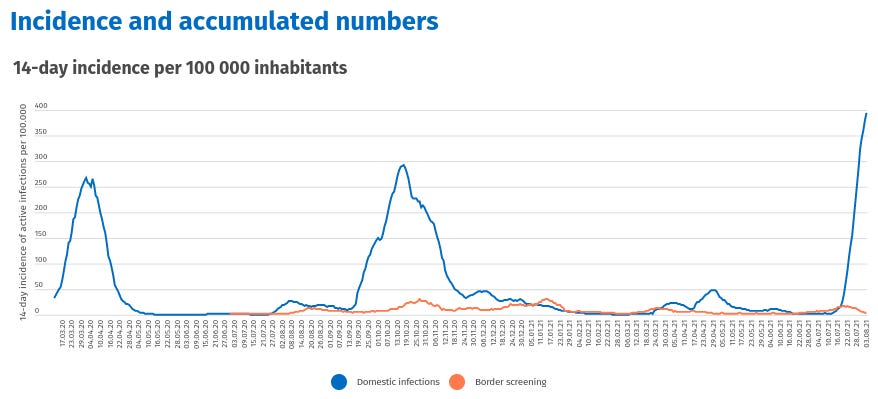
3. Iceland
While the overwhelming majority of Iceland‘s population has received COVID-19 jabs, the tiny island nation has recently seen a massive spike in infections, with most of them occurring through community transmission:
4. Massachusetts
In the recent outbreak in Barnstable County, Massachusetts – a state with a 69% ‘vaccination’ rate among those eligible for the jabs – the US Centers for Disease Control and Prevention (CDC) reported that:
74% of the 469 cases of COVID-19 occurred in fully-‘vaccinated’ people;
The Delta strain was identified in 90% of the specimens which were able to be genomically sequenced;
79% of the ‘vaccinated’ patients with a breakthrough infection were symptomatic;
4 of the 5 hospitalised patients were fully ‘vaccinated'(2 of whom had underlying medical conditions), while the sole unvaccinated hospitalised patient had multiple comorbidities;
There were no deaths reported;
There was no difference in cycle threshold (Ct) values on the real-time reverse transcription–polymerase chain reaction (RT-PCR) test between breakthrough cases and unvaccinated individuals, suggesting that the viral load is the same in fully ‘vaccinated’ people as in the unvaccinated and therefore that these breakthrough cases are just as likely to infect others as are unvaccinated people.
5. The Carnival Vista and HMS Queen Elizabeth
Outbreaks have occurred aboard several ships on which every single person on board was 'fully vaccinated': theCarnival Vista cruise ship and the UK Royal Navy's flagship, Queen Elizabeth as well as other warships in the fleet.
One wonders how those who wish to blame the unvaccinated for spreading SARS-CoV-2 are going to spin these spectacular failures.
‘Vaccinated’ people are as infectious as unvaccinated
‘Breakthrough’ cases of an infection that a person has been vaccinated against used to be called ‘vaccine failure’, back in the good ol’ days before English was replaced by Newspeak.
According to CDC, people who experience ‘breakthrough’ infections with the Delta variant of SARS-CoV-2 cases have just as high a viral load as unvaccinated people, and therefore are just as likely to be as infectious to others, as acknowledged by President Biden’s chief medical adviser, Dr Anthony Fauci:
“You can make a reasonable assumption that vaccinated people can transmit the virus just like unvaccinated people can.”
CDC reversal on indoor masking prompts experts to ask, ‘Where’s the data?’

[Source: Improving communications around vaccine breakthrough and vaccine effectiveness]
A study of breakthrough cases conducted in India found that fully-‘vaccinated’ health care workers who became infected with the Delta strain had higher viraI loads than those who became infected with other strains of SARS-CoV-2, and were also more likely to transmit the virus to others. Clearly, the ‘vaccines’ are ineffective against the now-dominant Delta strain:
“In vitro, the Delta variant shows 8 fold approximately reduced sensitivity to vaccine-elicited antibodies compared to wild type Wuhan-1 bearing D614G.”
SARS-CoV-2 B.1.617.2 Delta variant emergence and vaccine breakthrough
Equally clearly, forcing health care workers to accept these experimental injections is completely unjustifiable as it offers no benefit to their patients.
Herd immunity is impossible to achieve through the use of COVID-19 injections
Herd immunity – that is, indirect protection from infection that occurs when a sufficiently large proportion of a population is immune to a particular pathogen – can only occur when individuals who have either recovered from infection or been vaccinated against it have sterilising immunity – that is, a form of immunity that prevents infection from occurring.
The UK’s expert advisory board SAGE has acknowledged that
“[COVID-19] vaccines do not provide absolute sterilising immunity i.e. they do not fully prevent infection in most individuals.”
Scientific Advisory Group for Emergencies. Long term evolution of SARS-CoV-2
Furthermore, the jab-promoting Washington Post admits that currently available COVID-19 injections “are not designed [my emphasis] to create ‘sterilizing’ immunity.”
Think about that for a minute. If these injections are not designed to create sterilising immunity, then it’s been abundantly clear from the outset, to anyone with a functioning brain in their skull, that herd immunity could never have been achieved through their use.
SAGE also regards the likelihood of failure of current COVID-19 injections as “almost certain”, given the inevitability of ongoing changes in the genetic sequence of SARS-CoV-2.
The CDC also admits that because the current crop of COVID-19 vaccines are ineffective at preventing infection and transmission, there will inevitably be “more breakthrough and more community spread despite vaccination.”
And with the CDC estimating that there are 35 000 symptomatic infections per week occurring among 162 million ‘vaccinated’ Americans, that’s an awful lot of community spread.
To put it bluntly, there is no way in hell these injections can possibly achieve herd immunity, even if Australia – or any other country – achieves the 90% ‘vaccination’ rate touted by the likes of University of Melbourne professor of epidemiology Tony Blakely.
Honest epidemiologists – a breed that appears to be in short supply in Australia – are now acknowledging this unavoidable truth.
Professor Andrew Pollard, head of the Oxford Vaccine Group which developed the AstraZeneca injection that forms a key plank of Australia's vaccination strategy, has stated flatly that herd immunity is “not a possibility” given the heightened transmissibility of the Delta variant of SARS-CoV-2.
Þórólfur Guðnason, the Chief Epidemiologist of Iceland, a small island nation that has fully 'vaccinated' over 69% of its population and partially 'vaccinated' an additional 4.5%, has acknowledged that their aggressive vaccination program has not achieved herd immunity and will not be able to, given the failure of existing 'vaccines' to prevent infection and transmission.
Jeffrey Shaman, an epidemiologist at Columbia University, said:
“In some sense, vaccination is now about personal protection—protecting oneself against severe disease. Herd immunity is not relevant as we are seeing plenty of evidence of repeat and breakthrough infections [my emphasis].”
Covid-19: Delta infections threaten herd immunity vaccine strategy
Andrew Noymer, an epidemiologist at the University of California at Irvine, agreed:
“If the vaccinated can become infected and, we believe from other studies, potentially spread covid, then herd immunity becomes more mirage than oasis.”
Covid-19: Delta infections threaten herd immunity vaccine strategy
Now that it is clear that experimental COVID-19 injections cannot possibly offer Australia, or indeed any other country, an exit route from the pandemic, it’s time for politicians and health bureaucrats to stop their unwarranted and unacceptable intrusion into our private lives.
If, as Jeffrey Shaman stated, “vaccination is now about personal protection”, all individuals have the right to decide for themselves whether to accept or decline this form of ‘protection’, whether to choose another form of protection – for example through evidence-based prophylaxis and treatment protocols involving repurposed pharmaceuticals and nutraceuticals – or whether to simply go about their business as they have in every previous cold and flu season, doing their best to avoid falling ill and staying home to avoid infecting others if they do.
The state has no business interfering with citizens’ health and medical decision-making. That is a matter for each individual, in consultation with his or her doctor or other health care providers.
In next week’s post, I’ll present the evidence that COVID-19 injections are driving the development of more transmissible variants of SARS-CoV-2, and potentially laying the groundwork for much more serious outcomes of infection.