


Nine steps to optimal blood pressure
A comprehensive diet and lifestyle program is more effective than medication at reducing not just your blood pressure, but your risk of heart attack and stroke.

In last week's post, 5 reasons to think twice before taking blood pressure drugs, I highlighted the major adverse effects of some of the most popular classes of blood pressure-lowering medications that are taken by an estimated three million Australians, and hundreds of millions more throughout the world.
I also stressed that high blood pressure, or hypertension, is a 'silent killer' because it is "the leading global risk factor for cardiovascular, renal, neurological and ophthalmologic diseases".
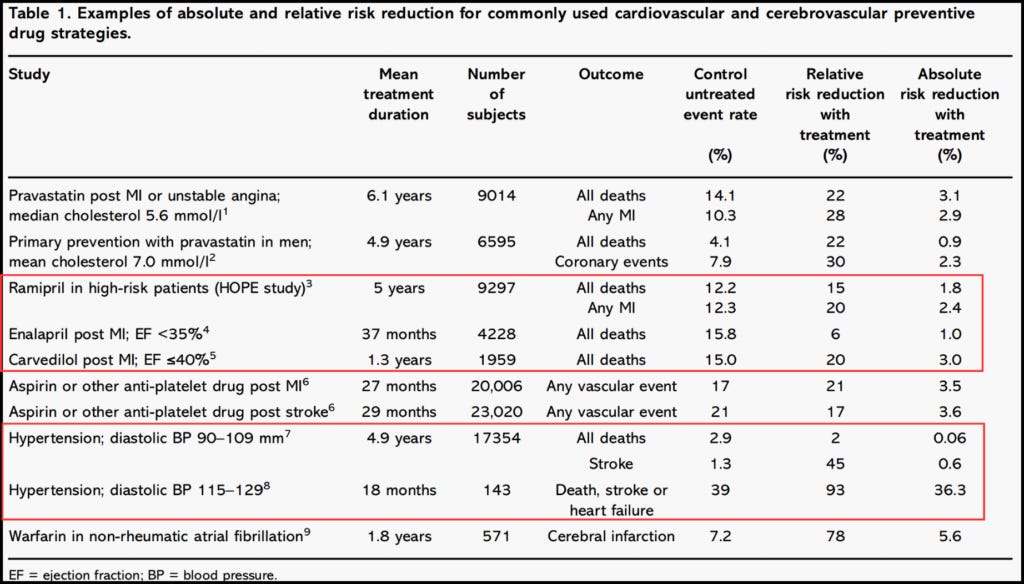
Antihypertensive drugs are fairly good at lowering blood pressure, but not so crash hot at reducing the risk of the hypertension-associated conditions that actually kill people... or disable them so much that they might wish they were dead. As you'll see from the table below, it's only when blood pressure is in the severely elevated range that antihypertensive drugs produce clinically meaningful reductions in outcomes that patients fear, such as death, stroke or heart failure:
The reason why antihypertensive drugs aren't particularly impressive at preventing hypertension-related conditions or reducing the risk of death, is that they do not address the underlying causes of elevated blood pressure.
What does address those causes? A comprehensive diet and lifestyle modification program. Here are the essential elements of such a program (and make sure you read all the way to the bottom, because I'm saving the most effective intervention until last):
1. Weight loss - or more specifically, visceral fat loss
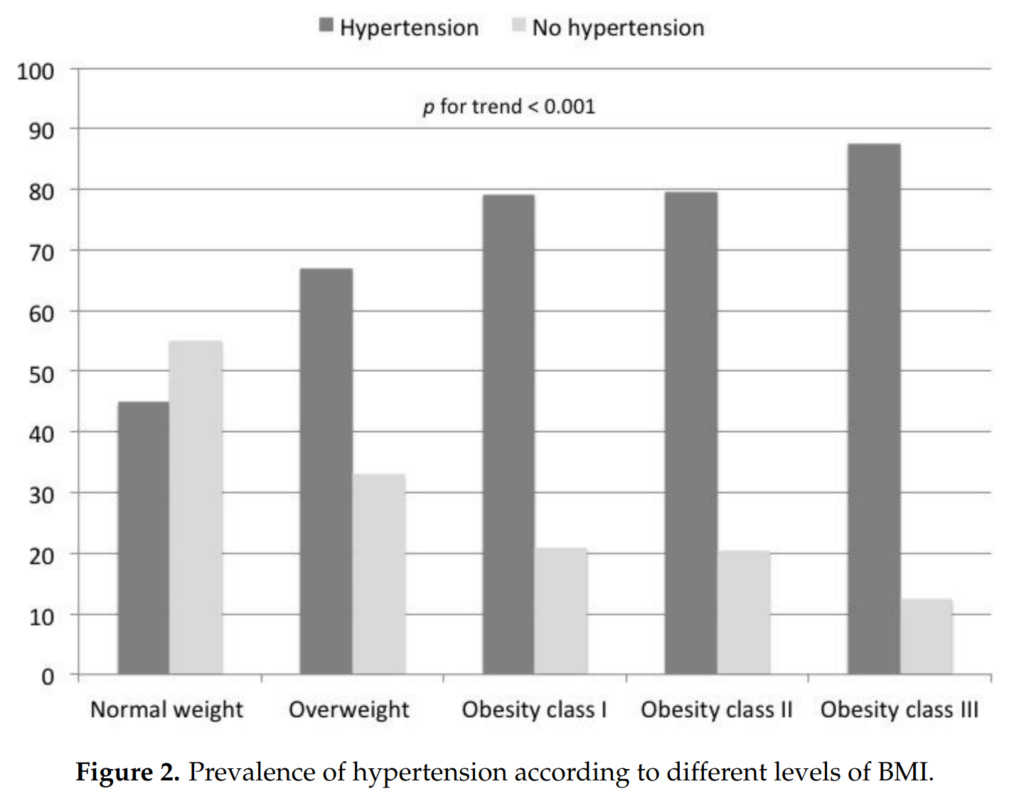
There is a strong and direct relationship between excess body weight and blood pressure. Even when using a relatively insensitive metric such as body mass index (BMI), which does not distinguish between lean and fat mass, it's abundantly clear that the larger one's body, the higher one's blood pressure.
For example, in a study conducted in7907 community-living Italian adults, hypertension was found in 45 per cent of participants with a BMI in the normal range (18.5–24.9 kg/m2), 67 per cent of those with a BMI in the overweight range (25.0–29.9 kg/m2), 79 per cent with obesity class I and II (30–39.99 kg/m2), and up to 87 per cent among participants with obesity class III (> 40 kg/m2)1.
Likewise, the Nurses’ Health Study II (NHS II) found that overweight and obesity was the strongest risk factor for developing hypertension:
"In this population, 40% of new hypertension cases (95% CI, 38-41%) could hypothetically be attributed to overweight or obesity (defined as a BMI ≥25 kg/m2), and 50% of new cases could hypothetically be attributed to a BMI ≥23.0 (95% CI, 49-52%)."
Diet and lifestyle risk factors associated with incident hypertension in women
A 2020 review came to even more dramatic conclusions, estimating that 65–78 per cent of cases of primary hypertension were attributable to obesity.
Gaining even small amounts of weight increases your risk of developing high blood pressure. For example, in the long-running Framingham Heart Study, participants who gained just five per cent of their body weight over four years of follow-up, had 20-30 per cent increased odds of hypertension. (That's a mere 3.5 kg weight gain for a 70 kg individual.)
Conversely, even modest weight loss can decrease blood pressure. In the Trials of Hypertension Prevention (TOHP) II study, overweight and obese participants who lost at least 4.5 kg and kept it off for the next 2.5 years, reduced their risk of developing hypertension by 65 per cent.
Excess body fat raises blood pressure via a number of mechanisms, many of them interlocking:
Overactivation of the sympathetic nervous system (the 'fear-fight-flight' arm of the autonomic nervous system);
Stimulation of the renin-angiotensin-aldosterone system (a complex system of hormones, proteins and enzymes that regulates blood pressure over the long term);
Alterations in cytokines (cell signalling molecules) derived from adipose tissue, such as leptin;
Insulin resistance; and
Changes to the structure and function of the kidneys.
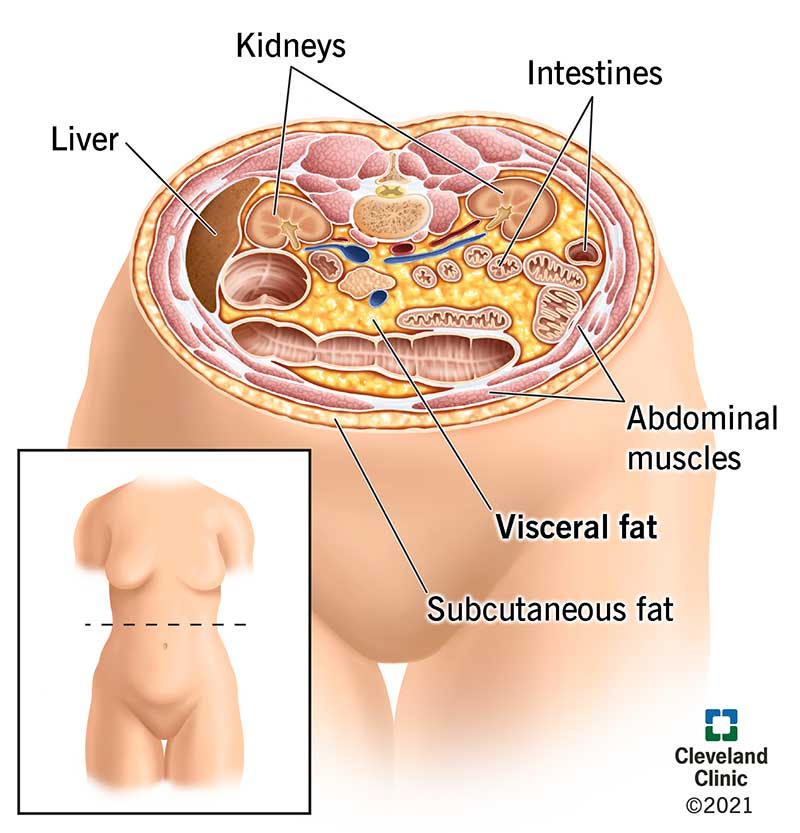
Most studies have found that accumulation of excess visceral adipose tissue (VAT - deep belly fat that wraps around, and intrudes into, your abdominal and pelvic organs) is more strongly associated with the development of hypertension than subcutaneous fat (the fat that accumulates just under the skin). Furthermore, VAT is strongly associated with treatment-resistant blood pressure, that is, blood pressure that remains elevated despite the use of three or more medications.
For example, men with newly detected, untreated essential hypertension (high blood pressure with no other medical cause) had 60 per cent more VAT than non-hypertensive men, as well as reduced insulin sensitivity. And in a study of 3363 Danish individuals, those with the most VAT (but not subcutaneous adipose tissue, or SAT) were the most likely to either have hypertension at baseline, or to develop it at five-year follow-up.
However, in a study of 1899 Japanese individuals, there was a stepwise increase in risk of hypertension with greater subcutaneous fat area in the abdominal region.
The bottom line is that if you're carrying excess body fat, especially around your midsection, you're at heightened risk of developing hypertension. And if you lose weight, you'll lower your blood pressure.
But there are many diets out there that are touted for weight loss and health improvement. Are any dietary patterns superior when it comes to taming hypertension?
2. Plant-forward diet
It's been known for nearly a century that vegetarians and vegans have lower blood pressure than omnivores, and that reintroducing meat to the diet of vegetarians raises their blood pressure. More recently, evidence has accumulated that people who get most or all of their calories from plant foods also have a lower BMI, less visceral adipose tissue and better insulin sensitivity. Following is a tiny sample of the many observational and experimental studies confirming these relationships (for many more, scroll down to the Discussion section of this study, and Chapter 8 of this book):
Observational studies:
Seventh Day Adventist (SDA) vegetarians have lower blood pressure and BMI than Mormons, who share the SDAs' religiosity and avoidance of alcohol, caffeine and tobacco, but not their dietary prescriptions. Vegetarian SDA men have lower blood pressure than omnivorous SDAs.
In the Oxford cohort of the European Prospective Investigation into Cancer and Nutrition (EPIC–Oxford), average systolic and diastolic blood pressures were found to be highest in meat eaters, lowest in vegans, and intermediate in fish eaters and vegetarians. 15 per cent of male, and 12.1 per cent of female meat-eaters reported that they had hypertension, vs 5.8 per cent of male and 7.7 per cent of female vegans. Among participants with no self-reported hypertension, meat-eating men's age-adjusted blood pressure was on average 4.2/2.6 mm Hg higher than vegan men’s. Meat-eating women had blood pressure 2.8/1.7 mm Hg higher than vegan women.
Like blood pressure, BMI was highest in the meat eaters and lowest in the vegans, with the fish eaters and vegetarians having similar and intermediate values, and this difference in BMI accounted for much of the difference in blood pressure between diet groups.
Saturated fat intake was positively associated with systolic blood pressure (SBP) in both sexes (i.e. the more saturated fat consumed, the higher the SBP), while the polyunsaturated:saturated fat ratio was inversely associated with blood pressure (i.e. the more polyunsaturated fat consumed in proportion to saturated fat, the lower the blood pressure).In the Coronary Artery Risk Development in Young Adults (CARDIA) Study, 4304 participants who were aged between 18 and 30 and had normal blood pressure at baseline, were followed for 15 years. After adjusting for a number of potential confounding factors, there was an inverse relationship between intake of plant foods (grains, fruit, vegetables, nuts, or legumes) and risk of developing elevated blood pressure. Those with the highest plant food intake had a 36 per cent lower risk than those with the lowest intake. BMI and waist circumference were also inversely correlated with plant food intake. That is, the more plants that went in the mouth, the smaller the waistline... even though participants who reported eating the most plants, had a higher self-reported energy (calorie/kilojoule) intake.
Conversely, consumption of red and processed meat was positively associated with the risk of developing elevated blood pressure, even after adjustment for possible confounding factors. There was a dose-response relationship - the higher the meat intake, the higher the blood pressure.The INTERMAP study found that for every 2.8 per cent increase in calories from vegetable protein, participants had 2.14 mm Hg lower systolic blood pressure, and 1.35 mm Hg lower diastolic.
Interventional trials:
In a randomised cross-over trial of staff at the Royal Perth Hospital, 59 healthy, omnivorous adults aged 25-63 years experienced a drop of 5-6 mm/2-3 mm Hg in their blood pressure after six weeks on a Seventh Day Adventist-style lacto-ovo-vegetarian diet. After resuming their regular omnivorous diet, their blood pressures rose once again. Participants were instructed to eat more if they noticed they were losing weight; hence there were no significant declines in body weight during the vegetarian diet.
500 adults (average age 58) participated in an intensive 12-day live-in program, during which they ate a low fat vegan diet. Despite most medications being stopped or reduced on the first day of the program, average blood pressure declined by 6 percent by the end of 12 days, with average falls of 9/4 mm Hg. Participants with the highest blood pressure at the outset of the program experienced the greatest declines; for those with higher than 140/90 mm Hg on entry, the average reduction in blood pressure was 17/13 mm Hg.
Men lost on average 2.5 kg by the 12th day, and women, 1 kg.21 strict vegetarians agreed to eat 250 g of beef per day for four weeks (substituting it for an equal calorie value of their usual fare), and then to revert to their normal vegetarian diet for another four weeks. During the meat-eating period, their average systolic blood pressure increased by three per cent.
Young healthy men, and healthy elderly men and women were fed a weight-maintaining high carbohydrate (roughly 68 per cent of energy intake), high fibre (70-100 g per day), low fat (14 per cent of daily energy) diet for one week. During this period, fasting glucose fell by 5 per cent, and insulin by 24 per cent, indicating improved insulin sensitivity. These effects were reversed in less than two weeks after participants resumed their normal diets.
3. Reduction of salt intake to evolutionarily appropriate levels, across the lifespan
According to the Australian Burden of Disease Study, roughly 21 per cent of the high blood pressure burden in Australia is due to a diet high in sodium. But what does 'high in sodium' mean?
In my previous article, A truly low salt diet lowers blood pressure as effectively as medicine – in one week, I discussed the pioneering work of S. Boyd Eaton and Melvin Konner, who launched the field of paleolithic diet research:
"In their seminal paper ‘Paleolithic nutrition: A consideration of its nature and current implications’, published in 1985, Eaton and Konner extrapolated from data gathered from extant hunter gather populations to estimate an average daily total intake of 690 mg of sodium in the paleolithic diet, with a potassium to sodium ratio of just over 16:1. Current average sodium intake is roughly ten times that of our ancient ancestors, and potassium intake now lags behind sodium – a complete inversion of the ratio between these two vital nutrients that shaped the development of the human kidneys, cardiovascular and endocrine systems."
A truly low salt diet lowers blood pressure as effectively as medicine – in one week
As a consequence,
"In every human population that uses salt, blood pressure rises with age, in stark contrast to communities that do not use salt – such as the isolated Yanomami people who inhabit the Venezuelan rainforest.”
A truly low salt diet lowers blood pressure as effectively as medicine – in one week
In that article, I also shared the results of a study that assigned participants aged 50 to 75 years, in random order, to one week on a high sodium diet (regular diet plus an additional 2200 mg of sodium per day in the form of bouillon cubes) and one week on a low sodium diet (approximately 500 mg of sodium per day). 25 per cent of participants had normal blood pressure, 20 per cent had medication-controlled hypertension, 31 per cent had uncontrolled hypertension, and 25 per cent had untreated hypertension. 73 per cent of participants experienced a drop in blood pressure when they switched from a high to a low sodium diet, with an average systolic blood pressure difference of 8 mm Hg between the high-sodium and low-sodium diet periods, which was, as the authors pointed out, “comparable with a commonly used first-line antihypertensive medication”.
I urge you to read that previous article in its entirety in order to grasp the wide range of adverse consequences of the virtually life-long overexposure to sodium that is typical of both developed and developing nations.
4. Alcohol reduction or abstinence
The risk of developing hypertension increases in a linear fashion with alcohol consumption - the more drinks per week, the higher the blood pressure.
Conversely, reducing alcohol intake brings blood pressure down. In a 2017 systematic review and meta-analysis, blood pressure decreased when people who drank more than two standard drinks per day reduced their alcohol consumption to near abstinence. The greatest reductions (average blood pressure decrease of 5.5/3.97 mm Hg) were seen in participants who drank six or more drinks per day, if they halved their intake.
5. Exercise and reduction in sedentary behaviour
Many people assume that they can offset time spent sitting on their butts by going to the gym or jogging. But it turns out that the more hours you spend in a seated position each day, the higher your systolic blood pressure, even if you also engage in intentional moderate-to-vigorous physical activity.
When it comes to intentional exercise, it turns out that isometric resistance - exercises that hold the body in one position, with muscles contracted but not changing length - is the most effective at lowering blood pressure. A 2013 systematic review and meta‐analysis of randomised controlled trials lasting four or more weeks, investigating the effects of exercise in healthy adults, found the following reductions in blood pressure :
Endurance training: 3.5/2.5 mm Hg
Dynamic resistance training: 1.8/3.2 mm Hg
Isometric resistance: 10.9/6.2 mm Hg
Combined training: 0/2.2 mm Hg
Greater reductions were seen in people who already had higher-than-ideal blood pressure. For example, after endurance training, hypertensive participants' blood pressure dropped by 8.3/5.2 mm Hg, but in prehypertensives, BP fell by only 2.1/1.7 mm Hg, and in normotensives, 0.75/1.1 mm Hg. In other words, exercise is a medicine that works best for those who need it most.

6. Sleep optimisation
Sleep deprivation, insomnia, sleep disruption due to restless legs syndrome, and obstructive sleep apnoea (OSA) all increase the risk of developing hypertension.
People who sleep less than 5 hours per night have up to a 72 per cent higher prevalence of hypertension, while in young adults, each hour of reduced sleep was associated with a 37 per cent increase in the odds of developing hypertension. On the other hand, sleeping for longer than 9 hours is associated with 30 per cent higher odds of hypertension, compared with individuals sleeping 7 to 8 hours. The 'sweet spot' for sleep does appear to be 7-8 hours per night, for adults.
If you suffer from OSA, you should listen to my interview with Dr Jessica Funk, and if you suffer from restless legs syndrome, tune into my Deep Dive webinar on this subject, on Tuesday, 27th February (or watch the replay) by joining my EmpowerEd membership program.
7. Ground flaxseed
In a double-blinded, placebo-controlled, randomised trial, 110 patients with peripheral artery disease consumed either 30 g of ground flaxseed, or placebo, each day for 6 months. At the end of the trial, patients who received flaxseed lowered their blood pressure by 10/7 mm Hg. Those who were hypertensive (systolic blood pressure ≥140 mm Hg at baseline) had a greater reduction in systolic blood pressure, of 15 mm Hg.
8. Hibiscus tea
In a randomised controlled trial comparing the effects of Hibiscus sabdariffa with the ACE inhibitor captopril on untreated hypertensives, a strong brew of hibiscus tea achieved equivalent reduction in blood pressure to the drug. Patients who drank hibiscus tea decreased their blood pressure by 15.3/11.3 mm Hg.
9. Water-only fasting
Remember that I urged you to read all the way to the bottom, because I was saving the best for last? Congratulations, you made it to the pot of gold at the end of the rainbow!
The most effective therapy for hypertension ever published in the medical literature is... drum roll please... medically-supervised water-only fasting, followed by refeeding with a low-fat, low-sodium, 100 per cent plant-based diet.
In a case series of 174 hypertensive people - that is, systolic pressure greater than 140 mm Hg and/or diastolic greater than 80 mm Hg - the average drop in blood pressure after a water-only fast of 10-11 days, followed by 6-7 days of refeeding, was 37/13 mm Hg. Those with stage 3 hypertension (systolic pressure greater than 180 mm Hg and/or diastolic pressure greater than 110 mm Hg) had an average reduction of a whopping 60/17 mm Hg at the conclusion of treatment. Compare this to the average reduction of 12/6 mm Hg achieved by standard antihypertensive drug treatment.
A second case series documented the effect of the same fasting-refeeding protocol on 68 people with borderline or stage 1 hypertension (systolic pressure between 120 and 139 mm Hg, and diastolic pressure less than 91 mm Hg). The average blood pressure reduction was 20/7 mm Hg, with the greatest decrease being observed for subjects with the highest baseline blood pressure.
Interestingly, the average decrease in blood pressure was not found to be significantly related to the amount of weight the subjects lost, indicating that fasting brings other blood pressure-lowering mechanisms into play. Reversal of insulin resistance and reduction of sympathetic nervous activity are strong contenders.
What if you aren't yet hypertensive?
Most people still believe that a blood pressure of 120/80 mm Hg is 'normal' and therefore healthy. But that's simply not true. A cohort study including 1457 participants without atherosclerotic cardiovascular disease reported that
"Beginning with a systolic blood pressure level of 90 mm Hg, there was a stepwise increase in the prevalence of traditional atherosclerotic cardiovascular disease risk factors, coronary artery calcium, and the risk of atherosclerotic cardiovascular disease. For every 10-mm Hg increase in systolic blood pressure, there was a 53% higher risk for atherosclerotic cardiovascular disease."
And a meta-analysis of nine prospective studies found that
"There did not appear to be any threshold below which a lower level of DBP [diastolic blood pressure] was not associated with a lower risk of stroke or CHD [coronary heart disease]."
In other words, when it comes to unmedicated blood pressure, the lower the better. So even if you have not been diagnosed with hypertension, prehypertension or elevated blood pressure, if you want to drive your risk of stroke, coronary heart disease and heart attack as low as you can get it, you should be adopting at least the first six measures outlined above, considering adding ground flaxseed and hibiscus tea to your diet, and exploring the benefits of periodic supervised water-only fasting2.
Finally, I put many hours into producing these posts. This one took me two solid days of researching and writing. If you feel you are getting value from reading my work, please consider a paid subscription:
Worried about your blood pressure and other markers of cardiovascular health? Confused about which medications you should be taking... or whether you should be on them at all? Apply for a Roadmap to Optimal Health Consultation and let's get the pressure down... for good!
Note that these BMI ranges are specific to Caucasians; the lower BMI cutoff of 25 kg/m2 for defining overweight in white adults translates to a BMI of 23.4 kg/m2 for black, 22.2 kg/m2 for Chinese, 22.1 kg/m2 for Arab, and 19.2 kg/m2 for South Asian adults.
Contact me if you want to be put in touch with an experienced fasting practitioner in Australia. US readers can contact TrueNorth Health Center or Fasting Escape.
Great article thanks Robyn, I came across this piece of info I found interesting in realation to blood pressure,
Ultraviolet-A Radiation (UVA) – Nitric Oxide + More
UVA (315-380nm) exists at a wavelength between UVB and visible light, and is able to reach deeper than UVB light but still only a few millimetres. UVA leads to the release of nitric oxide into the bloodstream which in turn benefits the cardiovascular and metabolic systems, and may offer other immunological benefits beyond those offered by nitric oxide. This vasodilatory effect enhances blood flow, lowers blood pressure and improves circulation.
https://tristanhealth.substack.com/p/why-you-can-never-replace-full-spectrum
Wow, this is fascinating.
30 G of flaxseed is a lot, but I mixed it into a salad with some quinoa, and it worked. Normally I would get that much in a week, so now I am doing this in a day. Fortunately I had quite a bit of flaxseed in the house.
Same for hibiscus tea, I have quite a bit in the house, always thinking it must be healthy, but I never started drinking it, so now I will. Thank you for all this excellent stuff!!!