


A truly low salt diet lowers blood pressure as effectively as medicine - in one week
How low should your salt intake go to tame high blood pressure?

As I've written in a previous article, 5 reasons to think twice before taking blood pressure drugs, high blood pressure is no trifling matter:
“High blood pressure (hypertension) kills. According to the Global Burden of Disease Study, it is the leading contributor to premature death and disability throughout the world. In fact, almost 20 per cent of early deaths across the world are linked to increased systolic blood pressure.
Having elevated blood pressure is the most significant risk factor for stroke and congestive heart failure; in fact, people with high blood pressure have four times the risk of stroke compared to people with normal blood pressure.
In addition, it accelerates the build-up of atherosclerosis, a fatty plaque lining the artery walls, and increases the likelihood that one of these plaques will rupture, triggering a heart attack or embolic (clotting) stroke.
High blood pressure also damages the kidneys, and since the kidneys play a huge role in regulating blood pressure, this damage generates a vicious circle of escalating blood pressure and organ destruction, which may eventually result in kidney failure and the need for dialysis.
The tiny arteries feeding the eyes can rupture due to the effects of constant high blood pressure, causing blurred vision and even blindness.
And high blood pressure accelerates dementia.”
Unfortunately, as I also explained in that article, antihypertensive drugs are no magic bullets. Each class of these medications has a distinct adverse effect profile. For example: thiazide diuretics elevate the risk of diabetes and arrthymias, calcium channel blockers increase older women's odds of dying of cardiovascular disease, and beta blockers bump up stroke risk in elderly patients.
While most people consider 120/80 mm Hg to be 'normal' blood pressure, your risk of atherosclerotic cardiovascular disease begins rising as soon as your systolic blood pressure goes north of 100 mm Hg. As you can see in the table below, in people who are not taking any blood pressure medications, those whose systolic blood pressure is between 100 and 109 mm Hg have roughly three times the risk of developing atherosclerotic cardiovascular disease as those with systolic blood pressure between 90 and 99 mm Hg:

Yet clinical practice guidelines instruct doctors to routinely prescribe antihypertensive drugs only when blood pressure is persistently above 160/100 mm Hg. Why?
Because in people with mild, or stage 1 hypertension (blood pressure ranging from 140/90 mm Hg to 159/99 mm Hg), the risks of antihypertensives outweigh the benefits.
In fact, as I discussed in High blood pressure: When drugs do more harm than good, a study which followed over 19 000 people with stage 1 hypertension and no history of cardiovascular disease (CVD) or CVD risk factors, for an average of 5.8 years, found no benefits of medication for reducing the risk of developing cardiovascular disease, or of dying... but an increased risk of excessively low blood pressure (hypotension), syncope (fainting, which can lead to head injury and bone fractures), electrolyte abnormalities and acute kidney injury.
This is why diet and lifestyle advice is recommended as first-line treatment for all people diagnosed with hypertension. And central to that advice is reducing salt consumption1.
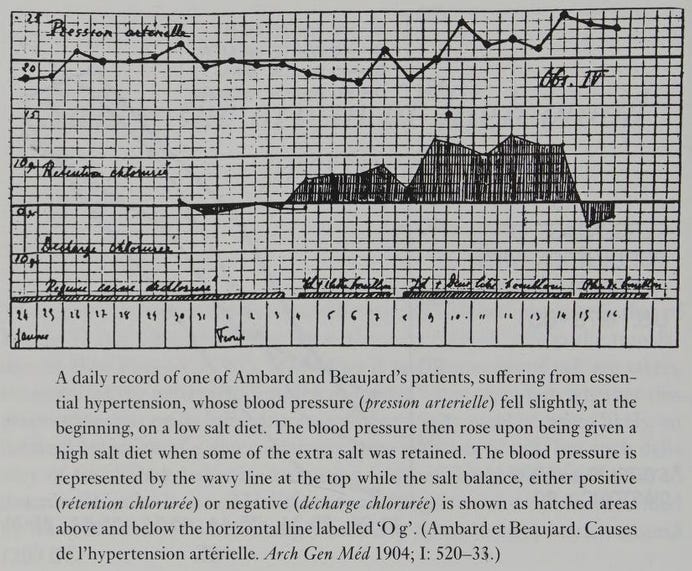
As the fascinating book Salt, Diet and Health (poetically subtitled Neptune's poisoned chalice: The origins of high blood pressure) relates, restriction of salt intake was first shown to lower blood pressure in people with essential hypertension - that is, those with no underlying medical cause of high blood pressure - in 1904. Two French doctors, Ambard and Beaujard, documented the effect of three diets with different salt levels on the blood pressure of six patients with essential hypertension. They established that on a low salt diet, less sodium was consumed than was excreted in the urine (negative sodium balance), and blood pressure fell. Conversely, when patients ate a high salt diet, they retained sodium, and their blood pressure increased.
Ambard and Beaujard's findings contradicted the dominant view that essential hypertension was caused by 'protein intoxication'. Hence they were largely ignored by the medical professsion until 1948, when Walter Kempner published a study of the effects of a very low salt diet on blood pressure, and related pathologies, in 500 patients. Kempner's 'rice diet' consisted solely of white rice and fruit, and contained less than 500 mg of sodium per day. His case series, and the mechanistic experiments which followed its publication, established beyond any doubt that dramatic reductions in salt intake cause substantial declines in blood pressure.
However, few people were prepared to stick to a diet as low in salt as Kempner's rice diet, and when diuretic drugs were developed in the mid-1950s, both doctors and hypertensive patients gratefully embraced them. Once again, Iow-salt diets were consigned to the dusty corners of medical libraries... until enough time passed for the adverse effects of diuretics, such as gout and erectile dysfunction, to become evident.
By the late 1960s, when my mother developed pre-eclampsia (a hypertensive disorder of pregnancy), innovative clinicians were once again open to considering the influence of salt intake on blood pressure. My mother's cardiologist sternly admonished her to throw away her salt shaker, advice that she dutifully followed without realising that 80 per cent of sodium intake is derived from pre-packaged foods (in particular, bread, processed meats and cereal products), rather than from salt added during or after cooking.
Beginning in the early 1970s, numerous studies demonstrated that reducing salt intake to between 3 and 6 grams per day - a far more moderate restriction than that utilised by Kempner - predictably lowered blood pressure, especially in elderly people and those with the highest blood pressure.
But recommendations to reduce salt intake to even this modest degree were met by pushback from the manufacturers of both salt itself, and the processed foods which rely on it for “the flavour burst” that helps to make their products hyperpalatable - and therefore, highly profitable.
Following the tobacco industry playbook, the Sultans of Salt set up purportedly independent organisations such as the Salt Data Centre, the Salt Information Bureau and the Salt Institute. Like the notorious Tobacco Institute, the names of these organisations were crafted to give the false impression of objectivity. Who could be opposed to having more 'data' or 'information' about salt? But in reality, their sole purpose was to run PR for their corporate backers by disputing the causal relationship between salt intake and hypertension, claiming that sodium restriction could be harmful to health, and misrepresenting research findings - including the results of Intersalt, "the largest ever international epidemiological comparative study in 52 centres worldwide representing both the rich and poor countries", to suit their paymasters' agenda.

In recent years, popular books and articles with titillating titles such as The Salt Fix: Why the Experts Got It All Wrong--and How Eating More Might Save Your Life and 'Pass the salt, please. It’s good for you' have rehashed the talking points of the salt industry front groups, seasoning them with a generous sprinkle of evolutionary biobabble.
Despite clear evidence that our ancient ancestors did not use salt - in fact, "languages before Greek and Sanskrit - the older of the Indo-European languages - had no word for salt" - the author of The Salt Fix implausibly insists that humans evolved on a high-sodium diet.
This argument would be most surprising to the OGs of paleolithic diet research, S. Boyd Eaton and Melvin Konner. In their seminal paper 'Paleolithic nutrition: A consideration of its nature and current implications', published in 1985, Eaton and Konner extrapolated from data gathered from extant hunter gather populations to estimate an average daily total intake of 690 mg of sodium in the paleolithic diet, with a potassium to sodium ratio of just over 16:1. Current average sodium intake is roughly ten times that of our ancient ancestors, and potassium intake now lags behind sodium - a complete inversion of the ratio between these two vital nutrients that shaped the development of the human kidneys, cardiovascular and endocrine systems. (As every student of physiology learns, the human kidneys are set up to conserve sodium as if it is gold dust, and to wantonly discard potassium, via the renin-angiotensin-aldosterone system.)
Not to be outstupided, the author of 'Pass the salt, please. It's good for you' quotes a professor of psychology who appears to believe that humans crave salt because it's good for us:
"'In biology, if something is attractive and we invest in gaining it, it must be beneficial, adaptive in evolutionary terms,' says Micah Leshem, a professor of psychology at Haifa University in Israel, who spent decades researching salt’s unique appeal."
By that logic, M&Ms must be a health tonic, and heroin a veritable panacea. Maybe ask an evolutionary biologist or a nutritional biochemist next time, rather than a psychologist?
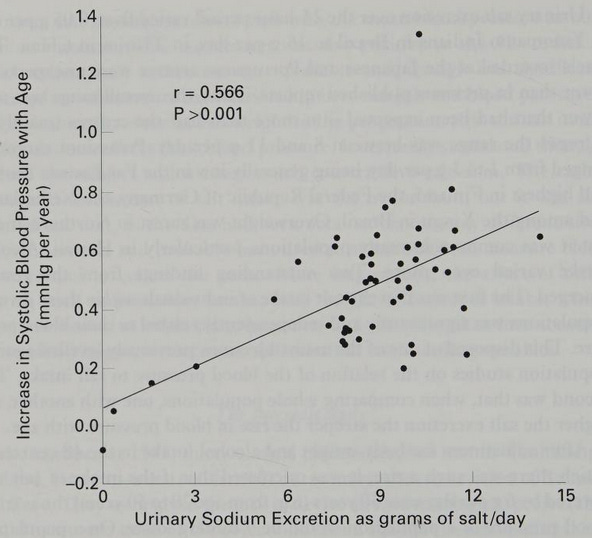
Recently, a new chapter in the ongoing salt saga was written, with the publication of a study titled 'Effect of Dietary Sodium on Blood Pressure: A Crossover Trial'. The authors sought to clarify inconsistencies in previous research on salt intake and blood pressure, especially in relation to 'salt sensitivity' - the impact of an abrupt change in salt intake or output on blood pressure. Not all people experience a spike in blood pressure when they acutely ingest salt. Critics of salt restriction argue that current sodium intake recommendations are unnecessarily restrictive for these 'salt resistant' individuals. Defenders of the recommendations point out that salt sensitivity and salt resistance are poor predictors of the long term response to a salt intake that is wildly in excess of our evolutionary exposure, and that in every human population that uses salt, blood pressure rises with age, in stark contrast to communities that do not use salt - such as the isolated Yanomami people who inhabit the Venezuelan rainforest. When examining the following graph, note that urinary sodium excretion directly reflects dietary sodium intake:
The researchers recruited 281 participants aged 50-75 years, from various U.S. cities, balanced across sex, race, and education. 213 completed the study, which entailed following, in random order, a high sodium diet (regular diet plus an additional 2200 mg of sodium per day in the form of bouillon cubes) and a low sodium diet (approximately 500 mg of sodium per day). Both diets were followed for one week.
Although only 46 per cent of participants were classified as 'salt sensitive' using established criteria, 73 per cent experienced a drop in blood pressure when they switched from a high to a low sodium diet:
"At the end of the first dietary intervention week, the mean systolic BP difference between individuals allocated to a high-sodium vs a low-sodium diet was 8 mm Hg (95% CI, 4-11 mm Hg; P < .001), which was mostly similar across subgroups of age, sex, race, hypertension, baseline BP, diabetes, and body mass index."
Effect of Dietary Sodium on Blood Pressure: A Crossover Trial
This blood pressure drop was, as the authors pointed out, "comparable with a commonly used first-line antihypertensive medication".
Let that sink in. Merely by cutting their sodium intake to a level comparable to that consumed by our ancient forebears, middle-aged to elderly people dropped their blood pressure by as much as they would if they had taken an antihypertensive drug. Colour me shocked that eating an evolutionarily appropriate amount of sodium is good for us!
The blood pressure response to switching between high and low sodium intakes was also roughly the same in people with normal blood pressure, hypertension controlled by medication, untreated hypertension, and uncontrolled hypertension. In other words, eating more sodium than our bodies are evolutionarily adapted to handle, has a universal impact on blood pressure. This has immensely serious implications, given the fact that, as I mentioned at the beginning of this article, high blood pressure is the leading contributor to premature death and disability throughout the world.
But was there a down side to cutting salt? 8 per cent of individuals reported mild adverse events (cramping and weakness) whilst on the low sodium diet. Bear in mind that 9.9 per cent suffered mild adverse events (primarily headaches, gastrointestinal discomfort, and oedema) on the high sodium diet. It's highly likely that, if participants persisted with the low sodium diet, even these minor symptoms would abate over time. After all, our paleolithic ancestors - and their even more primordial forebears - would not have been able to maintain high levels of physical activity in hot climates, if their low sodium intake caused them to cramp up and experience muscle weakness:
"Long before the appearance of Homo, australopithecines living in the heat of eastern and southern Africa would have encountered generations of natural selection pressure for the retention of diet-derived electrolytes, including sodium and chloride. Then, as now, under conditions of intense heat, sweating is essential for thermoregulation, yet sweating also facilitates electrolyte depletion with
potentially fatal physiological consequences. In the absence of supplemental dietary salt and given the usual vegetarian dietary regimen, we can surmise that the selection pressure for electrolyte conservation was both intense and consistent over evolutionary time. This selective pressure was undoubtedly activated very early in the history of our genera, and the individuals who were able to survive and reproduce in the face of this early and persistent selective constraint were likely to also evidence a spectrum of electrolyte conservation physiologies. Although a number of different physiological mechanisms (perhaps of diverse genetic origins) may have been expressed in these early humans, the overriding phenotypic effect would have been an emphasis on the retention of diet-derived electrolytes, particularly sodium, rather than their excretion. With stable and intense selective pressures against mechanisms of electrolyte depletion, adaptations consistent with the need for electrolyte conservation would have attained a high frequency among early humans. Given the duration of the gathering and hunting experience and our protracted existence in tropical biomes, an electrolyte-conserving phenotype can be thought of as the norm for our species."An Evolutionary Perspective on Salt, Hypertension, and Human Genetic Variability
Beyond blood pressure
If you're one of those people whose blood pressure does not decrease in response to a low sodium diet (remember, about 27 per cent of participants fell into this category), you may be thinking that you might as well just shake that salt cellar as much as you like. But the harms of salt ingestion go way beyond bumping up blood pressure: they actually change the amount of blood flowing to a crucial region in the brain.
That's what researchers found when they studied blood flow patterns in the brains of rats, after an acute salt load. The increased concentration of sodium set off a cascade of compensatory mechanisms, the end result of which was decreased blood flow and oxygen levels in the hypothalamus, a deep brain region involved in critical body functions including drinking, eating, body temperature regulation and reproduction.
The lead author of the study spelled out the implications of this unexpected finding:
"If you chronically ingest a lot of salt, you’ll have hyperactivation of vasopressin neurons. This mechanism can then induce excessive hypoxia, which could lead to tissue damage in the brain."
And then there's the immune-suppressing and pro-inflammatory effect of high sodium intake, which I discussed in Are you as-salting your immune system? In a nutshell (an unsalted one, of course), high concentrations of sodium impair the energy metabolism of immune cells' mitochondria – the tiny ‘power plants’ that convert glucose (blood sugar) into adenosine triphosphate (ATP), the universal currency of energy within all cells. Without sufficient ATP, immune cells are underpowered to fight off infection, and instead respond by spewing out inflammatory chemicals.
The most effective therapy for lowering blood pressure... and adjusting to a low-sodium diet
While dropping systolic blood pressure by 8 mm Hg in just one week is quite impressive, the most effective therapy for hypertension ever published in the medical literature is medically-supervised water-only fasting followed by refeeding with a low-fat, low-sodium, 100 per cent plant-based diet. In a case series of 174 people with systolic pressure greater than 140 mm Hg and/or diastolic greater than 80 mm Hg, the average drop in blood pressure after a water-only fast of 10-11 days followed by 6-7 days of refeeding, was 37/13 mm Hg. Those with stage 3 hypertension (systolic pressure greater than 180 mg Hg and/or diastolic pressure greater than 110 mg Hg) had an average reduction of 60/17 mm Hg at the conclusion of treatment.
A second case series documented the effect of the same fasting-refeeding program on 68 people with borderline or stage 1 hypertension (systolic pressure between 120 and 139 mm Hg, and diastolic pressure less than 91 mm Hg). The average blood pressure reduction was 20/7 mm Hg, with the greatest decrease being observed for subjects with the highest baseline blood pressure.
Although the blood pressure-lowering effect of water-only fasting is truly impressive, its impact on people's ability to adhere to a diet containing an evolutionarily-appropriate level of sodium may be even more impactful:
"In addition to providing for the rapid normalization of blood pressure and body weight, water-only fasting may have another, and perhaps more important, benefit. A period of water-only fasting is a period of sensory deprivation for taste nerves. This deprivation then results in a rapid sensitization to subtle taste stimuli... Present dietary patterns in industrialized societies use high-fat, high-sodium foods that not only promote hypertension, but also promote a palate that is generally intolerant of low-fat, low-sodium, high-potassium plant foods (Mattes, 1993). A period of sensory deprivation, such as water-only fasting, is a potentially powerful intervention for resensitizing taste nerves—and makes health-promoting fare much more palatable. This experience has been consistently observed in our clinic."
Medically Supervised Water-Only Fasting in the Treatment of Borderline Hypertension
In other words, fasting may be the only practicable way to 'reset' the acquired taste preference for salt back to a physiologically normal level. Just as populations that have never been exposed to salt manifest intense revulsion for it, after fasting, people find even lightly salted food absolutely disgusting. This has certainly been my own experience after fasting.
(Mandatory disclaimer: Fasting of this duration should only be done under qualified supervision. Contact me if you want to be put in touch with an experienced fasting practitioner in Australia.)
Conclusion
If you're reading this article, chances are that you've already woken up to the erroneous foundational premise of Western medicine, from which its litany of harmful dogmas and practices flow: allopathic medicine views the human body as inherently error-prone, and the symptoms of disease as manifestations of erroneous responses, that require correction through the application of drugs that interfere with biological processes, or procedures that remove or alter malfunctioning parts. While there is a small number of circumstances in which the body's responses are in error, the vast majority of 'diseases' are actually adaptations to environmental mismatch. High blood pressure is no exception:
"Given the pathological consequences associated with salt overload and toxicity, the sequelae of hypertension may be thought of as normal or expected responses to an abnormal environmental constraint, dietary salt overload."
An Evolutionary Perspective on Salt, Hypertension, and Human Genetic Variability
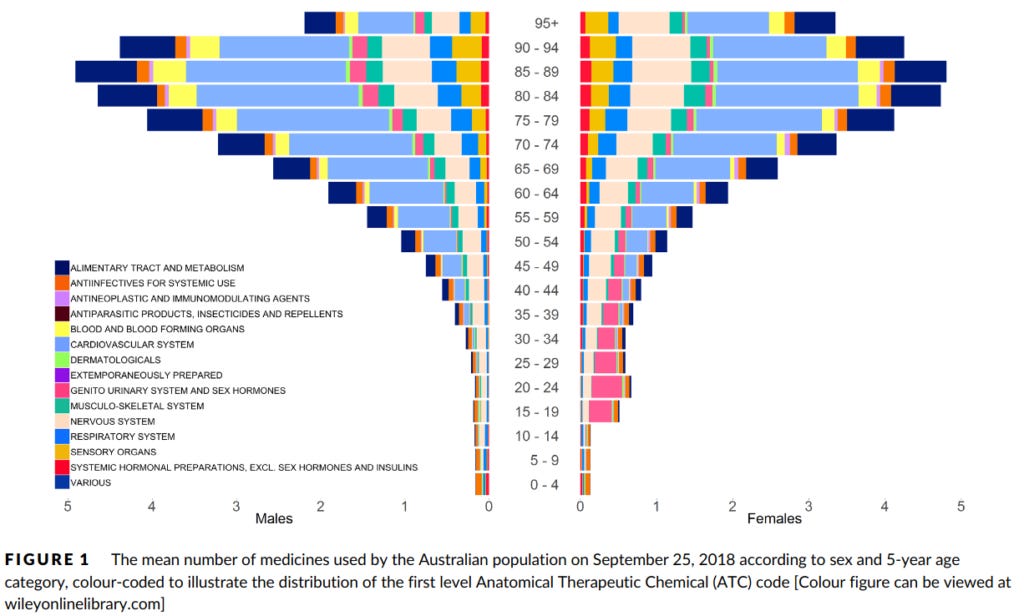
In plain English, if you consume more sodium than your body is evolutionarily adapted to handle, its attempt to adapt to the excess will cause you to manifest various signs and symptoms, including high blood pressure. If you are unwise enough to present to a conventional doctor, he or she will diagnose you with a disease condition - such as hypertension - and attempt to combat it with medications that interfere with your normal function. As a consequence of this interference, you will manifest 'side effects' which will most likely cause you to be prescribed more medications. This is how we end up with 45 per cent of Australians aged 70 years or over taking five or more medicines per day, and 8 per cent taking 10 or more.
Alternatively, you could tread the truly radical path: Take responsibility for your health, by removing the causes of illness - including excess sodium consumption - and putting in place the requirements for health - species-appropriate diet, adequate physical activity and sleep, time outdoors in nature, meaningful social contact and daily downshifting, and perhaps a supervised water-only fast if you really need to hit the 'reset' button. It's your choice... but if it's not an informed choice, you're not doing yourself any favours.
I'll leave the final word to the authors of Salt, diet and health. Neptune's poisoned chalice: The origins of high blood pressure:
"Our consumption of salt is now 10 to 20 times greater than 5000 years ago and it comes mainly from processed food. As the human body had become geared to conserve salt it found it difficult to dispose of this relatively sudden (in evolutionary terms) increase in salt intake. The result was a general rise in blood pressure. Those who had the greatest difficulty in getting rid of the excess salt had the greatest rise. A rise in blood pressure, however, damages the arteries and is the major cause of strokes and heart attacks, the commonest causes of death throughout the world."
Salt, diet and health. Neptune's poisoned chalice: The origins of high blood pressure
For information on my private practice, please visit Empower Total Health. I am a Certified Lifestyle Medicine Practitioner, with an ND, GDCouns, BHSc(Hons) and Fellowship of the Australasian Society of Lifestyle Medicine.
Although 'salt restriction' and 'sodium restriction' are often used interchangeably, salt refers to the compound sodium chloride, which comprises 40 per cent sodium by weight, and 60 per cent chloride.
Thanks for this Robyn, I did a lot of research on this when my Dad was prescribed various Blood Pressure lowering meds, the main point I seem to find as you briefly mentioned was it was the potassium to sodium ratio of the salt with respect to lowering blood pressure.
https://www.researchgate.net/publication/51615942_Feasibility_and_antihypertensive_effect_of_replacing_regular_salt_with_mineral_salt_-rich_in_magnesium_and_potassium-_in_subjects_with_mildly_elevated_blood_pressure
https://www.bmj.com/content/309/6952/436
As usual there a host of "side effects" with Blood Pressure medications, my dad also coincidentally started having skin problems when he started taking blood pressure meds.
https://www.health.harvard.edu/staying-healthy/medication-and-your-skin
https://www.epainassist.com/skin/what-blood-pressure-medications-cause-lichen-planus
https://www.webmd.com/skin-problems-and-treatments/psoriasis/qa/how-can-blood-pressure-meds-cause-your-psoriasis-to-be-worse
https://newsroom.unsw.edu.au/news/health/popular-high-blood-pressure-drug-linked-increased-skin-cancer-risk-older-australians
Can Taking Blood Pressure Pills Cause Itchy Skin? – World Of Medic (enteromedics.com)
The Itching Side Effect Of Blood Pressure Medication – World Of Medic (enteromedics.com)
Ask the doctor: Could my blood pressure pills be making me itch? | Daily Mail Online
Blood pressure medications: Types, side effects, and risks (medicalnewstoday.com)
There I was thinking bp around 110/70 was good !!!