Online health influencers claim that low cholesterol causes hormonal problems, damages your brain, and raises your risk of cancer and premature death. Are they right?
I've been doing a bit of debunking lately, haven't I? From deconstructing the everyone-should-be-taking-vitamin-D argument, to critiquing the ketogenic-diet-cures-cancer narrative, to blowing up the phytates-and-lectins-are-dangerous-antinutrients fables, I've spilled a whole lot of digital ink on debunking bad ideas that originate from the weird world of online health and nutrition 'influencers'1.
In case you're new here, and have jumped to the conclusion that this distaste for 'alternative health' woowoo means that I'm a Big Pharma shill, please read my articles on proton pump inhibitors, antidepressants, blood pressure pills, Ozempic and other GLP-1 agonists, and vaccines. I'm an equal opportunity bullsh*t buster. I just can't stand sloppy thinking - and there's plenty of that to go around in both the 'orthodox' and 'alternative' hemispheres of health care. I don't want to 'influence' you to believe, do or buy anything, and nor am I in favour of censoring other voices with whom I disagree. My aim is to help you hone your thinking skills so you can discern reliable information from codswallop2, whether said codswallop is ideologically-motivated or commercially-motivated (or both, as if often the case).
On that note, I think it's high time to debunk one of the major tropes currently being promoted by self-styled health experts: the notion that having a low serum cholesterol level is bad for your health, or, conversely, that you should be perfectly comfortable with having an elevated cholesterol level. It's not just the online bros who are peddling this nonsense; recently, I was consulted by a young, slim, active, healthy woman whose doctor had told her that her cholesterol level was 'too low', and that she should start eating coconut oil in order to raise it, because she didn't have enough cholesterol to produce hormones like oestrogen and progesterone 🤦.
Other arguments that the 'low-cholesterol-is-bad-for-you' crowd offer in defence of their position, is that the brain is mostly made from cholesterol, so low cholesterol causes depression, decreased cognitive performance and eventually, dementia; that low cholesterol levels increase the risk of cancer; and that people with low cholesterol have a higher mortality rate than people with higher cholesterol.
Cholesterol is a fatty, waxy substance which is found in all animal cells, both as a structural component of cell membranes, and a cell signalling molecule. It's also a precursor for the synthesis of steroid hormones including so-called 'vitamin D', testosterone, oestrogen and cortisol; and for bile acids, which are necessary for fat digestion and absorption of fat-soluble nutrients.
To summarise the key points arising from what I've just explained:
You have zero requirement for dietary cholesterol - that is, you do not need to eat foods that contain cholesterol in order to have enough cholesterol in your body. If you eat a lot of cholesterol, your liver and other cells will make less and absorb less of it, and if you eat little or no cholesterol, your body will make more and absorb more of it.
Your body can make cholesterol equally well from either carbohydrates or fats.
Your serum cholesterol level has absolutely nothing to do with the amount of cholesterol in your brain.
Thanks for reading Empowered! This post is public so feel free to share it.
Does low cholesterol increase risk of cancer, and death?
The 'high cholesterol is good for you' crowd are fond of pointing to studies that report higher risk of death in people with lower serum cholesterol levels as evidence for their claims. It is undeniable that among older people, those with the lowest cholesterol levels are the most likely to die in the next five years. But that is not because having low cholesterol increases your risk of death. It's because impending death reduces your cholesterol level. This is called reverse causation, and I discussed it in Never trust, always verify... even your allies:
"Reverse causation means (in this case) that declining cholesterol is the consequence of the deteriorating function that leads to death, rather than the cause of death. Anaemia, chronic inflammation, chronic renal and adrenal failure, nutrient deficiencies and hyperthyroidism (all common conditions in the final stages of life) all lead to reduced cholesterol production. Cancer, a leading cause of death, is also associated with reduced serum cholesterol, but cancer cells require cholesterol for growth and hence the relationship between low serum cholesterol levels and cancer is also attributable primarily to reverse causation."
It's been known since 1989 that cancer can begin to lower serum cholesterol levels up to ten years before it becomes clinically apparent. Most cancers grow slowly and do not cause any symptoms for years, or even decades. Hence,
"If you measure serum cholesterol levels in a large, randomly chosen population and then simply follow that population for 5 years—without intervention of any kind—there will be more cancer deaths in those who had the lowest cholesterol levels to begin with. Much of this (but perhaps not all) can be attributed to the fact that subclinical cancer is lowering the LDL levels in those subjects. This is especially true for leukemias and other cancers of the hemopoietic system but to some extent for all cancers. Tumor cells express high levels of the LDL receptor and catabolize LDL at a higher than normal rate (10). Thus, low LDL is the result, not the cause, of the cancer."
In that previous article, I also discussed the results of the Minnesota Coronary Experiment, which is often - completely erroneously - cited by sceptics of the hypothesis that elevated serum cholesterol plays a key role in atherosclerotic cardiovascular disease, as proof that lowering serum cholesterol through dietary means is harmful. The Minnesota Coronary Experiment randomised residents of one nursing home and six state mental hospitals to receive either a standard diet (controls), or a diet in which saturated fats - primarily from animal products - were almost entirely replaced with linoleic acid-rich corn oil. As mentioned in the previous article, the study was not able to be completed as planned because the deinstitutionalisation movement resulted in the closure of many mental hospitals, with the result that "almost three quarters of participants were lost within the first year and only about half of the remaining patients remained enrolled in the study for a full three years."
When data recovered from the experiment were published in 2016, it was found that for every 30 mg/dL (0.78 mmol/L) reduction in serum cholesterol, the risk of death was 22 per cent higher... BUT this was true both for the control group and the intervention group:
"In survival analyses (table 4), there was a robust association between decreasing serum cholesterol and increased risk of death, and this association did not differ between the intervention and control group (P>0.16 for all serum cholesterol×intervention interactions). Among both groups combined, a 30 mg/dL (0.78 mmol/L) decrease in serum cholesterol was associated with 22% higher risk of death from any cause (hazard ratio 1.22, 95% confidence interval 1.14 to 1.32) based on a Cox model adjusted for baseline serum cholesterol, age, sex, adherence to diet, BMI, and systolic blood pressure. The higher risk of death associated with decreased serum cholesterol seems to be driven by the subgroup aged ≥65. Among participants who were older than 65 at baseline, a 30 mg/dL decrease in serum cholesterol was associated with 35% higher risk of death (hazard ratio 1.35, 95% confidence interval 1.18 to 1.54), whereas among people aged under 65 at baseline there was no relation between the change in serum cholesterol and death (1.01, 0.88 to 1.16)." [my emphasis]
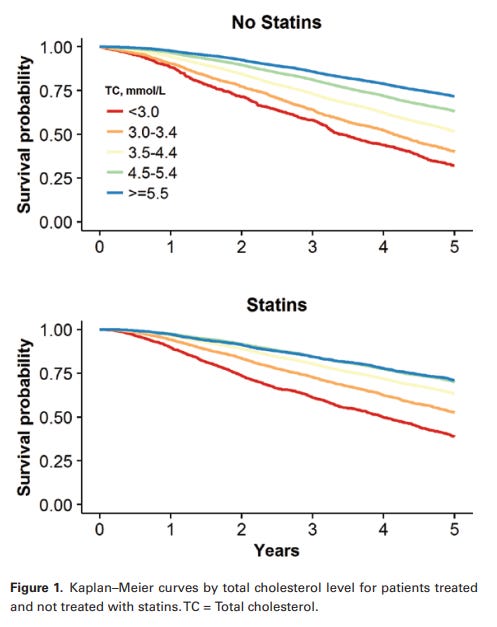
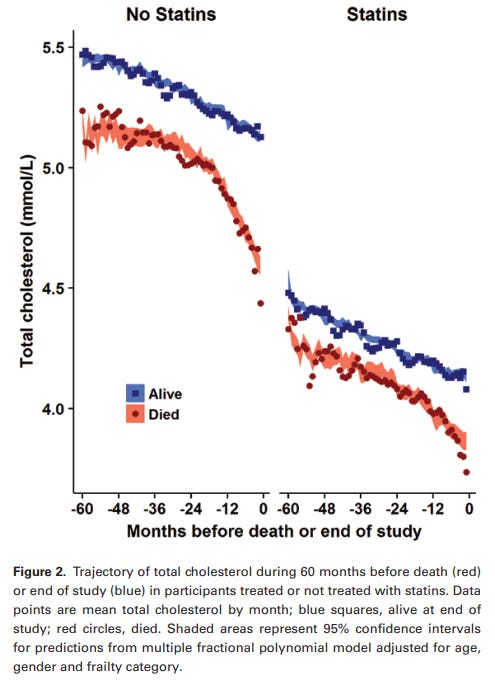
"The most plausible explanation for the association between declining cholesterol and increased risk of death, in older people but not in younger people, is the terminal decline in cholesterol that occurs as death approaches. A study called 'Trajectory of Total Cholesterol in the Last Years of Life Over Age 80 Years: Cohort Study of 99,758 Participants' found that elderly people with the lowest cholesterol levels were the most likely to die within the study period, regardless of whether they were treated with statins or not (and in fact those with declining cholesterol levels despite NOT being treated with statins were the most likely to die):
"Compared with TC [total cholesterol] values of 4.5-5.4 mmol/L, TC values <3.0 mmol/L were associated with higher mortality (statin treated hazard ratios 1.53, 95% confidence interval 1.43-1.64, p < .001; not treated, 1.41, 1.29-1.54, p < .001). A secular decline in TC values accelerated in the last 2 years of life. In the last quarter of follow-up, the adjusted odds of TC < 3.0 mmol/L for those who died, compared with surviving participants, were 3.33 (2.84-3.91, p < .001) for untreated and 1.88 (1.68-2.11, p < .001) for statin-treated participants."
"Conclusions: TC values show a terminal decline in the last years of life. Reverse causation may contribute to the association of lower TC with higher mortality in nonrandomized studies."
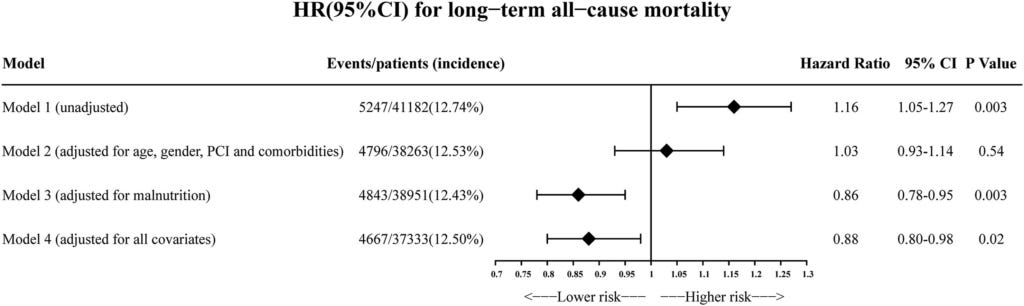
I mentioned previously that one of the contributing factors to terminal decline of serum cholesterol level is nutrient deficiency. In a study of over 41 000 patients with coronary artery disease admitted to a hospital in China, researchers found an inverse relationship between mortality and non-high-density lipoprotein cholesterol (non-HDL-C). That is, the lower the level of lipoproteins (cholesterol-transporting proteins) implicated in formation of atherosclerotic plaques, the higher the risk of death - exactly the opposite of accepted medical wisdom. Aha! So the cholesterol sceptics are right - low cholesterol is bad for your cardiovascular system! Not so fast: After accounting for the patients' age, sex, comorbidities and - most especially - their nutritional status, this relationship flipped:
Fig. 4. Unadjusted and adjusted HRs and 95% CIs for the primary end point (long-term all-cause mortality) of non-HDL-C < 2.2 mmol/L group vs. non-HDL-C ≥2.2 mmol/L group in CAD patients. Model 1: Unadjusted model. Model 2: Adjusted for age ≥75 years, sex, PCI and comorbidities including AMI, CHF, hypertension, diabetes mellitus, CKD, anemia, atrial fibrillation, COPD and stroke. Model 3: Adjusted for nutritional status. Model 4: Adjusted for all covariates: age ≥75 years, sex, PCI and comorbidities including AMI, CHF, hypertension, diabetes mellitus, CKD, anemia, atrial fibrillation, COPD, stroke and nutritional status. From Non-HDL cholesterol paradox and effect of underlying malnutrition in patients with coronary artery disease: A 41,182 cohort study.
In other words, CAD patients who had a non-HDL-C below 2.2 mmol/L because of advanced age, multiple illnesses, and malnutrition were odds-on to be meeting their maker before too long. But in patients who were younger, in better overall health, and were well-nourished, those with non-HDL-C below 2.2 mmol/L had a decreased risk of dying in the next few years compared to those whose non-HDL-C was above 2.2 mmol/L.
Serum cholesterol is not the only biomarker which undergoes terminal decline. Body mass index (a measure of weight adjusted for height), blood pressure and blood glucose, all show the same pattern of decreasing as we draw closer to death.
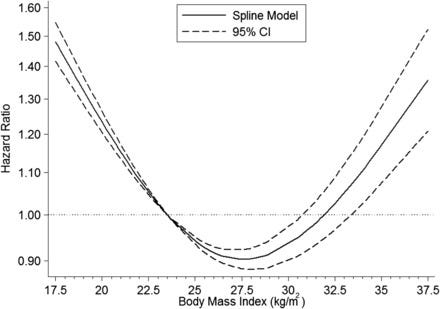
In a meta-analysis of 32 studies involving a total of almost 200 000 individuals aged 65 and older, with an average follow-up of 12 years, overweight people had the lowest mortality, while "all-cause mortality risk started to increase at a BMI of <23.0, which falls within the WHO healthy weight range for adults (BMI: 18.5–24.9)."
FIGURE 2. HRs (95% CIs) of all-cause mortality according to BMI for men and women aged ≥65 y. BMI was modeled with restricted cubic splines in a random-effects dose-response model. A BMI (in kg/m2) of 23.5 (most common midpoint for the reference BMI category) was used as the reference to estimate all HRs. The vertical axis is on a log scale. From BMI and all-cause mortality in older adults: a meta-analysis.
That "healthy weight range" is derived from tables devised by Metropolitan Life Insurance Company in the 1950s, after it observed that obese policyholders filed more claims than people who weighed less. But who takes out life insurance? Working-age adults. In young and middle-aged people, having a lower BMI is an indicator of good health in the present, and reduced risk of future disease. However, as people get older their body composition changes, such that they gain fat tissue and lose lean tissue (bone, muscle and vital organs). Hence, weight loss in older people is a red flag for frailty, which is a potent risk factor for death. Furthermore, many fatal illnesses including advanced cancer, chronic kidney disease, heart failure and chronic obstructive pulmonary disease, all cause weight loss.
In a retrospective analysis of over 229 000 patients with type 2 diabetes, the lowest risk of death was seen in those with an HbA1C (a measure of average level of blood sugar over the past 2-3 months) of 6–6.5% (42-48 mmol/mol), which is in the prediabetic range - that is, above what is considered healthy - and a systolic blood pressure of 130-140 mmHg, which is stage 1 hypertension. Values below and above these ranges were associated with higher risk of death.
So, should we all aim to increase our blood pressure and blood glucose levels in order to live longer? If our cholesterol-sceptic 'health influencers' were being consistent, that is exactly what they'd be recommending.
But, once again, not so fast! When the diabetic patients were stratified by age and degree of comorbidity, it was only the oldest patients - those aged over 72 years - who had less risk of death with higher blood pressure and glucose levels. The explanation, once again, is terminal decline.
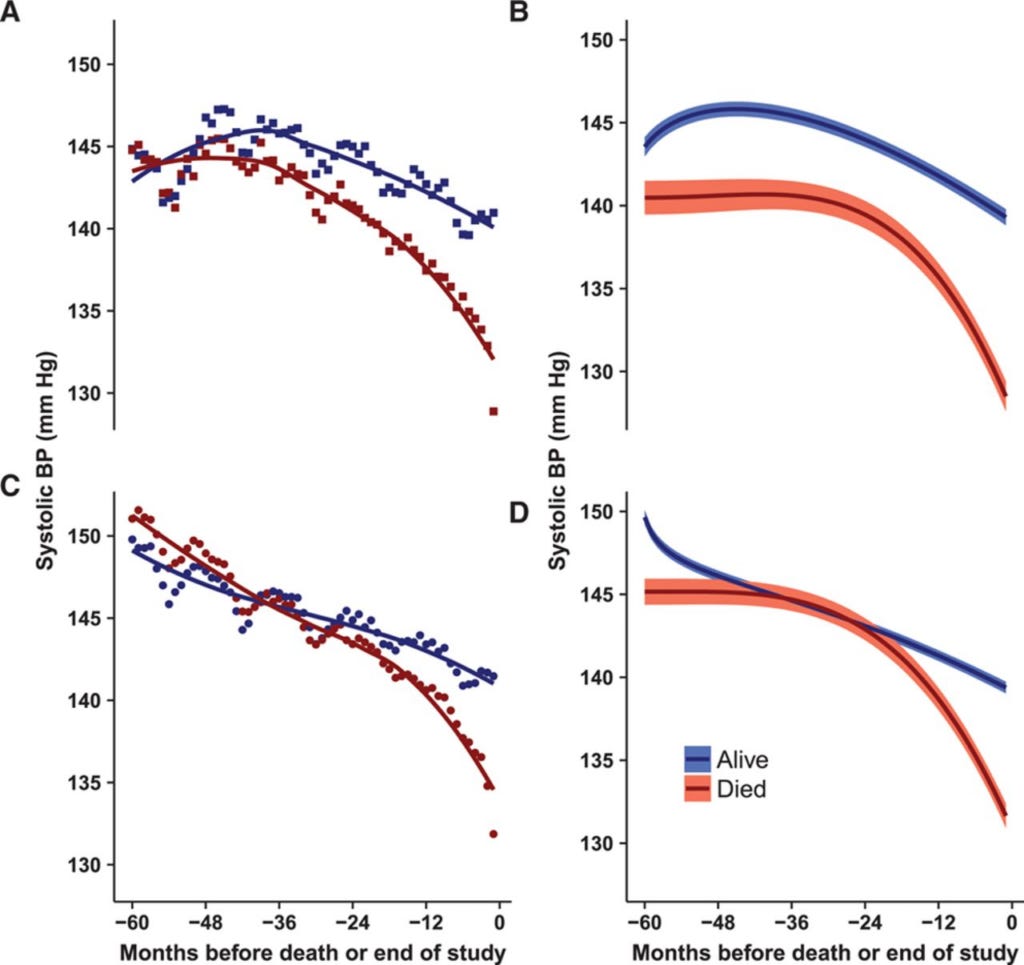
While blood pressure rises with age in industrialised societies, as we approach death it begins to decline. When the blood pressures of over 144 000 people aged over 80 were followed for up to five years, or until their death, a very consistent pattern emerged: blood pressure declined in the final five years of life, accelerating dramatically in the final two years of life, regardless of whether patients were on antihypertensive medication - C and D in the following figure - or not - A and B; notice how the red lines (signifying patients who died during the follow-up period) all fall off a cliff in the final 24 months:
Figure 1. Trajectory of systolic blood pressure during 60 months before death (red) or end of study (blue). Left, Mean SBP by month: (A) squares, not treated; (C) circles, treated with antihypertensive medications. Right, Predictions (95% confidence intervals) from multiple fractional polynomial model adjusted for age, sex, calendar year, and frailty category: (B) not treated; (D) treated with antihypertensive medications. From Systolic Blood Pressure Trajectory, Frailty, and All-Cause Mortality >80 Years of Age: Cohort Study Using Electronic Health Records.
The fact that the steep decline in blood pressure in the final years of life occurs whether patients are on blood pressure-lowering medication or not indicates that terminal decline is the only rational explanation for this phenomenon; the authors confirmed this by noting that "there was no evidence of intensification of antihypertensive therapy in the final 2 years of life."
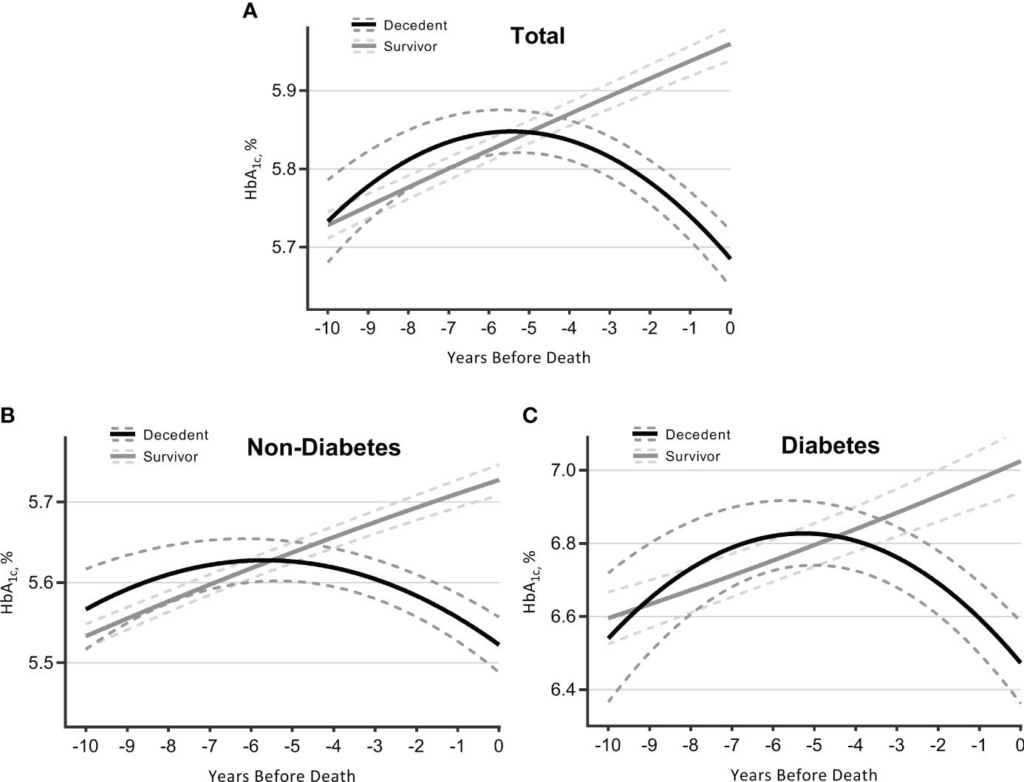
Likewise, when the HbA1C of over 10 000 adults aged over 50 was tracked for an average of almost nine years, those with the highest HbA1C at baseline had the highest risk of dying, but as the study progressed, a lower HbA1C was a harbinger of impending death:
"HbA1c trajectory first rose and then terminally declined at an accelerated rate as death approached."
Figure 2 Trajectories of HbA1c over 10 years before death (decedents, n = 3,070) or end of follow-up (survivors, n = 7,338). Estimated mean values were from linear mixed-effect models for total sample (A), participants without diabetes (B), and those with diabetes (C). Analyses were adjusted for sex, age at time 0, race, marital status, education, smoking, drinking, body mass index, physical activity, hypertension, diabetes [not for figure (B) or (C)], heart diseases, multimorbidity score, survival status, time terms (time and time 2), and interactions of survival status and time terms. HbA1c, glycated hemoglobin. From Terminal trajectory of HbA1c for 10 years supports the HbA1c paradox: a longitudinal study using Health and Retirement Study data.
Summing up, low serum cholesterol (total or non-HDL) does not increase the risk of cancer, or death. The association between low serum cholesterol and death from cancer or other natural causes is attributable to terminal decline, a phenomenon that is also observed with weight/body mass index, blood pressure and blood glucose.
So what cholesterol level should I aim for?
At this point, you might be wondering what your serum cholesterol level should be, for optimal health and longevity. According to Dr Loren Cordain, the OG of the Paleolithic Diet movement, the optimal range for LDL cholesterol is... wait for it... 50 to 70 mg/dl or 1.3-1.8 mmol/L - roughly half that of carnivore diet-promoting Paul Saladino who revealed in an interview that his LDL-C is 130 mg/dl (3.4 mmol/L).
In a 2004 article, Cordain and co-authors pointed out that
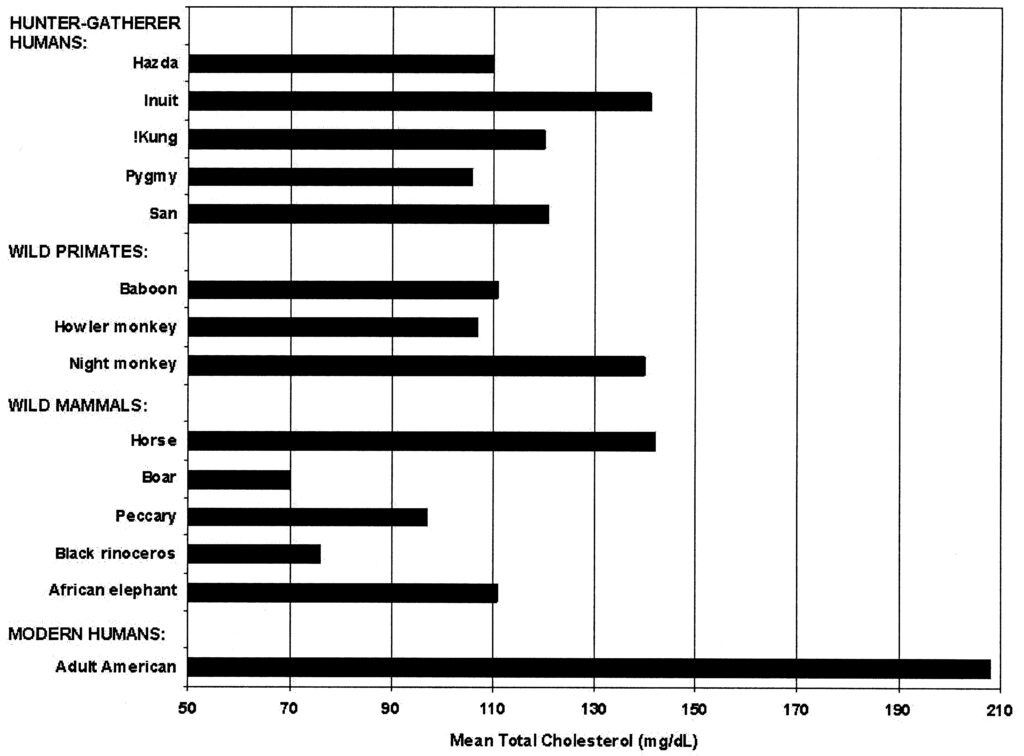
"The average total cholesterol level in American adults today is 208 mg/dl (corresponding to an LDL of approximately 130 mg/dl) (13). In this case, average is not normal because atherosclerosis is present in up to 40% to 50% of women and men by age 50 (14). Atherosclerosis is endemic in our population in part because the average person's LDL level is approximately twice the normal physiologic level (Fig. 1).
Huh. Isn't that interesting? The man who literally wrote the book that launched the movement which spawned today's crop of meat-munching health influencers says that Paul Saladino's LDL cholesterol level is unnaturally high, unhealthy, and abnormal for the species. Now, it's not that I think that every word that Loren Cordain spoke is gospel truth; I think his advocacy for a high-protein, meat-heavy diet neglects the reality of evolutionary trade-offs. But I'll say this much for him: his thesis was at least based on careful study of the diets and biometrics of hunter-gatherer peoples, not just-so stories like those spun by Saladino and his ilk.
Take-home messages
I have enormous sympathy for people who are fed up to the back teeth with 'experts'. I understand why so many are turning away from professionals who are seen to be identified with 'the system', with all its manifold conflicts of interest and deep corruption, and instead getting their health advice from people they encounter on social media. There are serious flaws in the education system and credentialling mechanisms of doctors, dietitians and other health professionals, and these flaws are valid grounds for distrust.
But having gone through that education and credentialling system myself, I can tell you one major benefit that it offers - at least for students who, like me, are enraptured by human biology and biochemistry: It equips you to sniff out bullsh*t. And bullsh*t is the stock in trade of many, if not most, of the 'health influencers' with large online audiences. Maybe they know they're trafficking in bullsh*t, and maybe they don't. Few of my classmates shared my passion for the bioscience subjects, and I wouldn't be surprised if most had forgotten everything they ever learned about the biosynthesis and regulation of cholesterol, and the compartmentalisation of brain and peripheral cholesterol, by the time they graduated. I'll bet the same phenomenon applies to doctors, including those promoting the ridiculous notions that I've debunked in this article.
It may seem overwhelming, if you're a layperson with no educational background in the relevant scientific disciplines, to be saddled with the responsibility for fact-checking every claim you read or hear online. But, as I wrote in Unpacking the ‘ketogenic diet cures cancer’ myth: Part 2, we now have this handy-dandy thingo called 'the internet', which allows you to type a question such as "does low cholesterol cause cancer?" into a search engine, identify articles from reputable sources (i.e., not some rando's blog), and then use AI tools such as Brave's built-in AI assistant, Leo, to parse highly technical information into a relatively easy-to-understand summary. Yes, it will cost you anywhere from a couple of minutes to several hours, to verify each claim. But that effort it might just save your life.
And finally, this post has taken me approximately 20 hours to research and write. It takes much more time to debunk statements that aren’t true, than it does to spout them! I make all my posts freely available to all readers, because I believe we all deserve access to information that helps us to take greater control over our health. But I rely on my small core of paid subscribers to provide this service to those who genuinely can’t afford it.
Empowered! is a reader-supported publication. Without the generous support of my paid subscribers, I could not continue to bring you this important information.
For information on my private practice, please visit Empower Total Health. I am a Certified Lifestyle Medicine Practitioner, with an ND, GDCouns, BHSc(Hons) and Fellowship of the Australasian Society of Lifestyle Medicine.
Think about that word for a moment. When someone is booked for drunk driving, they're charged for being 'under the influence' of a mind-altering substance. An 'influence operation' is an organised attempt to affect people's beliefs and behaviour towards a specific aim. When you 'follow' an 'influencer', how is your mind being altered, and for what (and whose) aim?
Once again, thanks for your research on cholesterol. I just recently viewed a video on YouTube, Nutrition Made Simple by Dr Gil Carvahlo, covering this exact topic; do high blood pressure, high blood glucose, high cholesterol numbers indicate longer life?
Anecdotally, my cholesterol numbers don’t seem have any relation to lifestyle. When I retired from the Navy at 42, I was fit(ran, lifted weights, cycled, swam), 7% body fat, healthy(cholesterol was 116), yet I didn’t eat what we would call a healthy diet today. Three years later cholesterol was up to 118. In the years before and after, my levels varied between 120-170, without changes in diet or lifestyle. I don’t know what those numbers are now as I haven’t had blood work done. As Dr Tom Cowan says, “there’s a 100% cure for high cholesterol, which is never to do the test again.” I relate this to say I can read many things, which in the end help me little. Which brings me to the questions you didn’t address; what is high? What is low? What is normal?
I read some of the links you referenced and here is what I garnered:
a)Dietary cholesterol content has little impact on plasma cholesterol (including LDL-cholesterol).
b) It is thus legitimate to question whether dietary cholesterol itself (inde-pendently of plasma cholesterol levels) has a relationship (either a simple, statistical association or a causal relationship) with the risk of CVD
c) On the basis of these data, one can conclude that if dietary cholesterol does lead to an increased risk of CVD, that risk is low. The clinical implication is thus negligible.
It seems that society is bifurcated. How can two people, or two groups look at the exact same data and draw two opposite conclusions. Seed oils are bad. Seed oils are good. Linoleic acid is bad. No, it’s good. Carbs are bad. Carbs are good. Eggs are bad. No, they’re good. This bifurcation isn’t just with nutrition and health. It’s everything. I’m not even talking about influencers. That’s just a euphemism for con artist. My opinion is that all the numbers we are given as to what is healthy are just that - numbers. Statistics.
Fascinating to watch the 'experts' from different frames of reference pushing a specific perspective on so many different issues Robyn. Often on the latest bandwagon it seems.
Discerning the truth around real health choices and optimal lifestyle etc can be challenging to say the least. Appreciate your perspective and encouraging people to think Robyn. Loved your critical thinking posts!




Once again, thanks for your research on cholesterol. I just recently viewed a video on YouTube, Nutrition Made Simple by Dr Gil Carvahlo, covering this exact topic; do high blood pressure, high blood glucose, high cholesterol numbers indicate longer life?
Anecdotally, my cholesterol numbers don’t seem have any relation to lifestyle. When I retired from the Navy at 42, I was fit(ran, lifted weights, cycled, swam), 7% body fat, healthy(cholesterol was 116), yet I didn’t eat what we would call a healthy diet today. Three years later cholesterol was up to 118. In the years before and after, my levels varied between 120-170, without changes in diet or lifestyle. I don’t know what those numbers are now as I haven’t had blood work done. As Dr Tom Cowan says, “there’s a 100% cure for high cholesterol, which is never to do the test again.” I relate this to say I can read many things, which in the end help me little. Which brings me to the questions you didn’t address; what is high? What is low? What is normal?
I read some of the links you referenced and here is what I garnered:
a)Dietary cholesterol content has little impact on plasma cholesterol (including LDL-cholesterol).
b) It is thus legitimate to question whether dietary cholesterol itself (inde-pendently of plasma cholesterol levels) has a relationship (either a simple, statistical association or a causal relationship) with the risk of CVD
c) On the basis of these data, one can conclude that if dietary cholesterol does lead to an increased risk of CVD, that risk is low. The clinical implication is thus negligible.
It seems that society is bifurcated. How can two people, or two groups look at the exact same data and draw two opposite conclusions. Seed oils are bad. Seed oils are good. Linoleic acid is bad. No, it’s good. Carbs are bad. Carbs are good. Eggs are bad. No, they’re good. This bifurcation isn’t just with nutrition and health. It’s everything. I’m not even talking about influencers. That’s just a euphemism for con artist. My opinion is that all the numbers we are given as to what is healthy are just that - numbers. Statistics.
Fascinating to watch the 'experts' from different frames of reference pushing a specific perspective on so many different issues Robyn. Often on the latest bandwagon it seems.
Discerning the truth around real health choices and optimal lifestyle etc can be challenging to say the least. Appreciate your perspective and encouraging people to think Robyn. Loved your critical thinking posts!