


Diving down the low-carb rabbit hole - Part 1
Is Dr Paul Mason a disruptive genius, a dissembling showman, or... something else?

NOTE: I originally published this as an unfinished, work-in-progress article. I’ve now converted it into Part 1 of a two-part series. Please read (or reread it) before you read Part 2. Note that I’ve added some material to this part since I originally published it.
My last two articles on high blood pressure (5 reasons to think twice before taking blood pressure drugs and Nine steps to optimal blood pressure) have generated some lively discussion in the Substack comments section. I received some pushback from people who believe that a ketogenic, or carnivore, diet is the best way to reduce blood pressure, reverse insulin resistance and prevent cardiometabolic disease.
I welcome polite and respectful debate, as we all benefit from having our opinions and beliefs challenged through the presentation of contradictory evidence. However, I do set some ground rules: Firstly, I respect people's personal experience when it comes to their various dietary experiments, but such anecdotes do not constitute scientific evidence. If a particular diet seems to be working for you, I'm very happy for you - but don't expect me to abandon the recommendations that I currently make, based on over three decades of studying the research literature, and conducting my own clinical practice, because of your n=1 experiment. And secondly, I'm not generally interested in watching videos of my readers' favourite dietary gurus, because at least 90 per cent of these videos are simply storytelling, unrooted in any actual evidence.
However, one of my readers was so insistent that I would learn life-changing new information if I viewed some videos of one such guru, Dr Paul Mason, that I decided to watch the recommended presentation. I wouldn't say I learned anything new, but I did come away impressed by how many distortions, half-truths and assorted logical fallacies a single individual can pack into a 26 minute lecture.
The presentation is called Decoding Atherosclerosis: The clotting theory and seed oil toxicity. I'm going to share time stamps and quotes (taken from the YouTube transcript, and corrected where required), along with my critiques.
0:16: "Now today I'm going to challenge everything you know about this disease which is atherosclerosis."
My regular readers might recall that this claim - or any other variation of “everything the ‘experts’ tell you about nutrition is wrong" is one of the red flags of nutritional charlatanry that I highlighted in Debunking nutrition myths: A how-to guide. It's not that there aren't any controversies in nutrition science; of course there are, as in other disciplines. And it's not that it's impossible for a large percentage of researchers in a given field to be operating within a paradigm that turns out to be either completely wrong, or inadequate to explain observable phenomena; Max Planck's observation that science advances one funeral at a time is as true today as it ever was.
But I am immediately on my guard when I hear anyone claim that 'everyone else is wrong and I'm right'. Extraordinary claims require extraordinary evidence. Let's see if Dr Mason delivers that extraordinary evidence.
0:24: "You've been told that high LDL cholesterol coats the inside of blood vessels in much the same way that the drain gets clogged by fat and this is just absurd."
I agree that this is an absurd claim, but I don't know of any researcher in the field of atherosclerosis who makes it. Doctors may use silly analogies like this with their patients, when they either don't have a sufficiently solid grasp of the aetiology of atherosclerosis to explain it properly, don't have time to explain it properly, or believe they need to 'dumb down' their messaging as their patients won't understand a complex explanation. But this is not how atherosclerosis is described in the scientific and medical literature.
Mason is simply employing a straw man argument, perhaps to build a bond between him and his audience, so they can feel superior to the ignorant masses (including many doctors) who believe stupid ideas.
0:35: "High LDL cholesterol levels are in fact associated with longevity. The overwhelming finding of this systematic review of 19 cohort studies with more than 68,000 participants found that people with higher LDL cholesterol levels lived longer."
The study that informs Mason's claim is 'Lack of an association or an inverse association between low-density-lipoprotein cholesterol and mortality in the elderly: a systematic review'. This paper suffers from multiple serious methodological weaknesses, including the following:
No study hypothesis, predefined statistical analysis or study protocol was provided, making it difficult for readers to check the authors' work.
The authors used an extremely limited search strategy in which only one electronic database (PubMed) was searched, using a small number of text words: "‘lipoprotein AND (old OR elderly) AND mortality NOT animal NOT trial’". The use of this limited search strategy put the review at high risk of bias for omitting relevant studies (more on this soon).
263 of the 282 full text articles initially identified were excluded from analysis, and the reasons for excluding these studies were not given.
Criteria for including or excluding studies were inconsistently applied, suggesting cherry-picking to suit the authors' preconceptions.
For example, one of the exclusion criteria was "studies without multivariate correction for the association between LDL-C and all-cause and/or CV [cardiovascular] mortality". Yet a study which contributed two-thirds of the total number of participants included in this analysis, did not include such multivariate correction and hence should have been excluded. Interestingly, this study found that "statin treatment after inclusion [in the study] provided a survival benefit," undermining the claims of the authors of the systematic review that "the benefits from statin treatment have been exaggerated".1
Conversely, this study was excluded from the analysis, supposedly because "it included the same individuals as in a previous study" (this one). However, the excluded study, which presented more detailed statistical analysis, reached a different conclusion to the included study - namely, that there was no association between LDL-cholesterol and mortality.
And this study, which fulfilled the inclusion criteria, was not mentioned at all. This ignored study found that, even in very elderly people, those with high LDL-cholesterol due to genetic factors had higher all-cause mortality: "In longitudinal analysis, high GRS [genetic risk score] was associated with increased all-cause mortality in individuals > 90 years, with a 13% increased risk in individuals with the highest LDL GRS (P-trend = 0.043)." Conversely, genetic disposition to low LDL-cholesterol was "associated with familial longevity."No details of the statistical analysis methods used in the paper were provided.
Participant-level data was not available to, or was not sought by, the authors. Instead, they relied on limited, aggregated and inconsistent information from published sources, an approach which introduces potential bias into the analysis.
No statistical adjustments were made to account for potential confounding factors that could either mask an association between LDL-C and mortality, or falsely suggest such an association when there is none. The major such potential confounding factor, as the authors of the systematic review themselves acknowledged, is statin treatment:
"It is worth considering that some of the participants with high LDL-C may have started statin treatment during the observation period. Such treatment may have increased the lifespan for the group with high LDL-C. However, any beneficial effects of statins on mortality would have been minimal because most statin trials have had little effect on CVD and all-cause mortality, with a maximum reduction of mortality of two percentage points."
No reference was given for these claims, and no accounting for the potential impact of statins was attempted.No methodological quality assessment was presented for each included study, however, independent analysis of this paper by the Centre for Evidence-Based Medicine concluded that "All the included cohort studies provide data that would be judged as low quality according to GRADE criteria."
For deeper insight into the serious methodological flaws with this paper that Dr Mason relies upon to support his claim that having elevated LDL-cholesterol is good for you, I urge you to read the Centre for Evidence-Based Medicine's detailed critique.
And you'll find an even more detailed critique of another paper with the same lead author (Uffe Ravnskov), which repeats some of the same arguments and adds several more, here.
Finally, this paper analysed data from three prospective studies of over 80,000 men aged 18-39 years, and followed up for up to 34 years, and found
"a continuous, graded relationship of serum cholesterol level to long-term risk of CHD, CVD, and all-cause mortality, substantial absolute risk and absolute excess risk of CHD and CVD death for younger men with elevated serum cholesterol levels, and longer estimated life expectancy for younger men with favorable [i.e. lower] serum cholesterol levels."

1:25: "LDL particles can be found in atherosclerotic plaque. So does that mean LDL causes atherosclerosis? No. Just because two factors coexist doesn't mean that one causes the other."
Here, Mason employs the fallacy of suppressed evidence, by failing to mention the multiple strands of research - observational, experimental, and Mendelian randomisation (genetic risk) studies - that support the argument that there is a causal relationship between elevated LDL-cholesterol (or, more strictly speaking, between apolipoprotein B-containing lipoproteins) and atherosclerotic cardiovascular disease.
As just one example of this voluminous evidence-base, below are figures from a systematic review and meta-analysis of intervention trials of statins and non-statin agents (including diet changes) that are intended to lower LDL-cholesterol. For every 1 mmol/L (38.7 mg/dL) reduction in LDL-cholesterol achieved by the use of statins, the relative risk for major vascular events was reduced by 23 per cent. Per 1 mmol/L reduction in LDL-cholesterol level achieved via nonstatin interventions that work primarily via upregulation of LDL receptor expression, the relative risk for major vascular events dropped by 25 per cent.
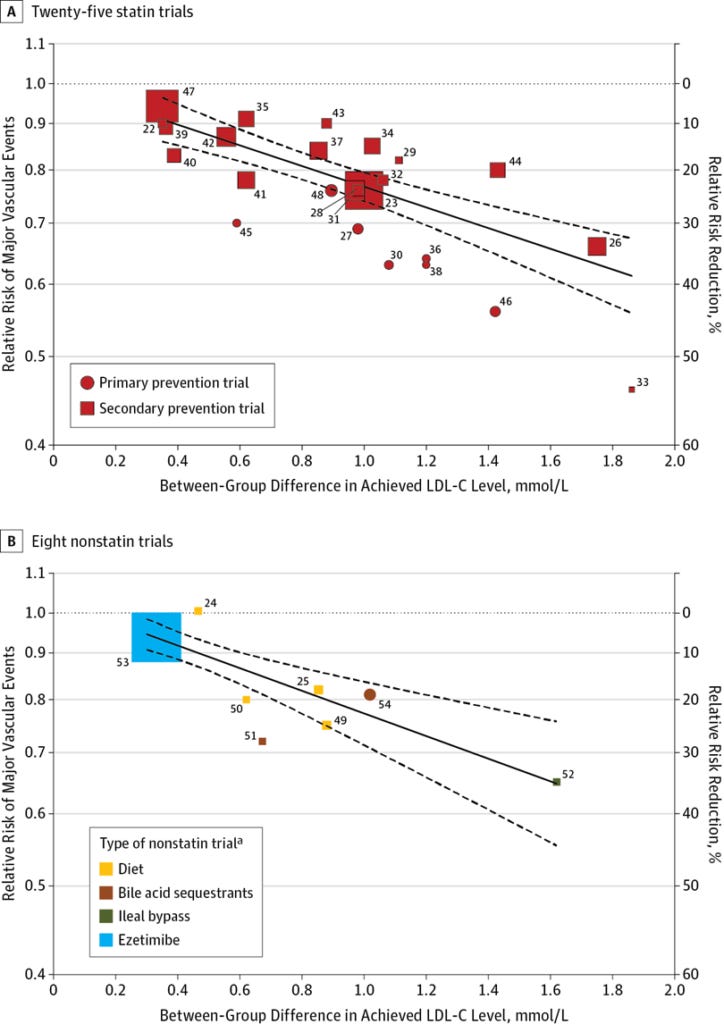
Mason's hand-waving argument that 'correlation doesn't equal causation' just doesn't stand up to the evidence that interventions which lower circulating LDL-cholesterol, also reduce atherosclerosis-related events.
1:44: "The fact is, as shown by this paper, 75% of patients hospitalised with heart attack have normal levels of LDL."
The paper Mason is referring to is this one. The authors of this paper state that "Prospective epidemiological data have suggested that the relationship between LDL and CHD [coronary heart disease] is log-linear, with a relative risk set at 1.0 for LDL of 40 mg/dL." That is, the risk of coronary heart disease starts to go up once LDL-cholesterol rises above 40 mg/dL (1.03 mmol/L). But in this study, only 17.6 per cent of patients hospitalised for coronary artery disease had LDL-cholesterol below 70 mg/dL. It's unclear how Mason derived the "75%" figure, or what he means by "normal levels of LDL". Suffice it to say that pretty well all of the patients in this study had an LDL-cholesterol level above the known threshold for coronary heart disease.
As the godfather of paleolithic nutrition, Dr Loren Cordain, pointed out in a 2004 paper,
"Evidence from hunter-gatherer populations while they were still following their indigenous lifestyles showed no evidence for atherosclerosis, even in individuals living into the seventh and eighth decades of life (15,16). These populations had total cholesterol levels of 100 to 150 mg/dl [2.6-3.9 mmol/L] with estimated LDL cholesterol levels of about 50 to 75 mg/dl [1.3-1.9 mmol/L]. The LDL levels of healthy neonates are even today in the 30 to 70 mg/dl [0.8-1.8 mmol/L] range... In fact, modern humans are the only adult mammals, excluding some domesticated animals, with a mean LDL level over 80 mg/dl [2.1 mmol/L] and a total cholesterol over 160 mg/dl [4.1 mmol/L] (15,16)(Fig. 1). Thus, although an LDL level of 50 to 70 mg/dl seems excessively low by modern American standards, it is precisely the normal range for individuals living the lifestyle and eating the diet for which we are genetically adapted."
Optimal low-density lipoprotein is 50 to 70 mg/dl: Lower is better and physiologically normal
And, finally, LDL-cholesterol levels decline in the 48 hours following a heart attack, so the LDL-C measured in these patients was not representative of their usual levels anyway.
1:54: "Rather we've got compelling evidence that the root cause of heart disease is actually this: a blood clot, or more specifically, thrombosis. Essentially atherosclerosis is the result of blood clots forming inside blood vessels... blood clots are not just made of red blood cells; they also contain platelets and fibrin which forms the strands that bind the clot together, and these two have been found buried deep inside atherosclerotic plaques, and the lipid heart hypothesis does not explain this at all."
The fact that blood clots occur within atherosclerotic plaques is not exactly ground-breaking to cardiovascular disease researchers, who've been documenting such clots for decades. And you know something that causes more blood clots to form? Elevated LDL-cholesterol.
This paper describes multiple mechanisms by which elevated LDL-cholesterol increases blood clotting, including stimulating platelet activation and raising the levels of fibrinogen, the precursor to fibrin.
And as described in this paper, LDL-cholesterol increases the formation of thrombi (blood clots) in the microvasculature of the heart muscle. The clots are formed when von Willebrand factor activates platelets, causing them to clump together. von Willebrand factor can also bind red blood cells and crosslink to fibrin. And wouldn't you know it, patients with hypercholesterolaemia have higher plasma levels of von Willebrand factor.
Finally, people with a rare genetic condition called abetalipoproteinaemia, that results in a lack of all apolipoprotein B-containing lipoproteins (including LDL-cholesterol), have reduced platelet activation.
Hence, the lipid heart hypothesis, in fact, explains the presence of blood clots within atherosclerotic plaques perfectly well, since elevated LDL-cholesterol increases the propensity of the blood to form clots, via multiple mechanisms.
6:19: "Phytosterols, this fake form of plant cholesterol, is readily detected in atherosclerotic plaques."
Phytosterols are not a "fake form of cholesterol"; they're a naturally-occurring compound in plant foods, which our paleolithic ancestors consumed in significant amounts. And while it is true that phytosterols are detectable in atherosclerotic plaques, a comprehensive review of the use of plant sterols as functional foods concluded that at present, it is not clear whether plant sterols increase, decrease, or have no effect on atherosclerotic cardiovascular disease.
6:42: "Fortunately for most of us our bodies can reject most of the plant sterols that we consume with only about 1% actually being absorbed and assimilated into our tissues. Some people aren't this lucky however; they have a disease called sitosterolaemia and that means that rather than absorbing only 1% they can absorb between 15 and 60% and the consequence of this can be dire... premature severe atherosclerosis is the norm in this condition where you absorb too much plant sterol. Despite this, phytosterols are often lauded for their ability to reduce cholesterol levels and we have products like this which deliberately contain added plant sterols which are promoted for cardiovascular health despite there being approximately zero evidence of cardiovascular benefit and plenty of evidence of harm."
Once again employing the fallacy of suppressed evidence, Mason fails to mention that the "some people" with sitosterolaemia comprise a grand total of 110 reported cases worldwide. To steel man Mason's argument, genetic studies suggest that the condition may be less rare than previously believed, with roughly 1 in 200,000 people having genetic mutations that adversely affect their phytosterol metabolism. Even so, the relevance of the dire consequences of phytosterol intake in people with sitosterolaemia to the 199,999 out of every 200,000 people who don't have this rare condition is, to put it mildly, unclear. And to reiterate my earlier point, it is not true that there is "plenty of evidence of harm" of supplemental phytosterol intake; the evidence is currently inconsistent.
For the record, I do not recommend the use of phytosterol supplements or functional foods (such as margarines) fortified with phytosterols. These are highly-processed foods (or food components) to which our species has no history of exposure - unlike the phytosterols found naturally in plant foods.
8:35: "This study looked at the impact of butter, olive oil and coconut oil on cholesterol in the blood and it found that both coconut and olive oil caused a drop in LDL levels, in my opinion due to the plant sterol content, and this was despite the coconut oil containing 94% saturated fat. It still led to a drop in LDL. This is a clear repudiation of the claim that saturated fat increases LDL."
The study Mason is referring to is this one. Once again, he omits crucial information, namely that the decline in LDL-cholesterol levels in people assigned to eat coconut oil or olive oil, failed to reach statistical significance. (This occurs when there is a wide spread in responses i.e. some participants' LDL-cholesterol went up, and others’ went down.) Importantly, while participants were given 50 g per day of their assigned oil or fat, and instructed to incorporate it into their usual diet or use it as a supplement, daily total fat intake in the coconut oil group rose by 29 g, in the olive oil group by 28 g, and in the butter group by only 14 g. This indicates that participants were partially substituting the oils or butter for their regular cooking fats and spreads, but there was less substitution in the butter group. The authors did not attempt to account for these variations in the source of fat intake, in their analysis. Furthermore, the authors attributed the difference in impact on LDL-cholesterol of the two highly-saturated fats - coconut oil and butter - not to the phytosterol content of the former, but to the substantial variance in fatty acid profiles of these two fats. Coconut oil predominantly contains lauric acid whilst butter is high in palmitic and stearic acids, which have been shown in previous research to raise LDL-cholesterol more than lauric.
9:10: "Now one of the major reason seed oils contribute to atherosclerosis is that their polyunsaturated chemical structure contains unstable bonds which are prone to oxidation. Basically all the seed and vegetable oils you see in stores are oxidised."
Note that Mason has at no point in this presentation provided evidence that "seed oils contribute to atherosclerosis". It's a rhetorical trick to insert this claim into his talk at this point, to imply that he has proven a point that in fact, he has not.
Now, it's undeniable that polyunsaturated vegetable oils are prone to oxidation. However, the impact of oxidised LDL-cholesterol on coronary heart disease risk is outweighed by the total number of atherogenic (that is, apolipoprotein B-containing) lipoproteins, including subtypes of LDL-cholesterol.
For example, this study followed 18,140 men and 32,826 women for six years, and found that "circulating oxLDL [oxidised low-density lipoprotein], measured with antibody 4E6, is not an independent overall predictor of CHD [coronary heart disease] after adjustment of lipid markers and is less predictive in development of CHD than apoB [apolipoprotein B] and TC/HDL-C [total cholesterol over high-density lipoprotein-cholesterol] ratio." To paraphrase Slick Willy himself, it's the apoB, stupid.
Even more importantly, this study showed that as LDL became more oxidised, it was less able to penetrate the inner lining of the artery wall to form an atherosclerotic plaque. So Mason's focus on oxidation products formed within the blood is misplaced; it's what's happening in the artery wall that matters, when it comes to atherosclerotic cardiovascular disease.
9:47: "The story for blood oxidation products becomes even more interesting when we have subjects with poor blood sugar control. The two left columns represent subjects with normal blood glucose levels and the right column those with poorly controlled diabetes, meaning they've got high blood sugar levels, and you can see the blood oxidation product level is much higher in the poorly controlled diabetics. Furthermore the blood oxidation products lasted for nine times longer in these subjects, being detected in the circulation for 3 days compared to 8 hours for the healthier subjects. So what, you might ask, is the problem with oxidation products in the blood? The answer is atherosclerosis, as in oxidative stress in the blood triggers blood clotting or thrombosis, which as you now know is the source of atherosclerosis."
This is the study Mason is referencing, and here is the graph:
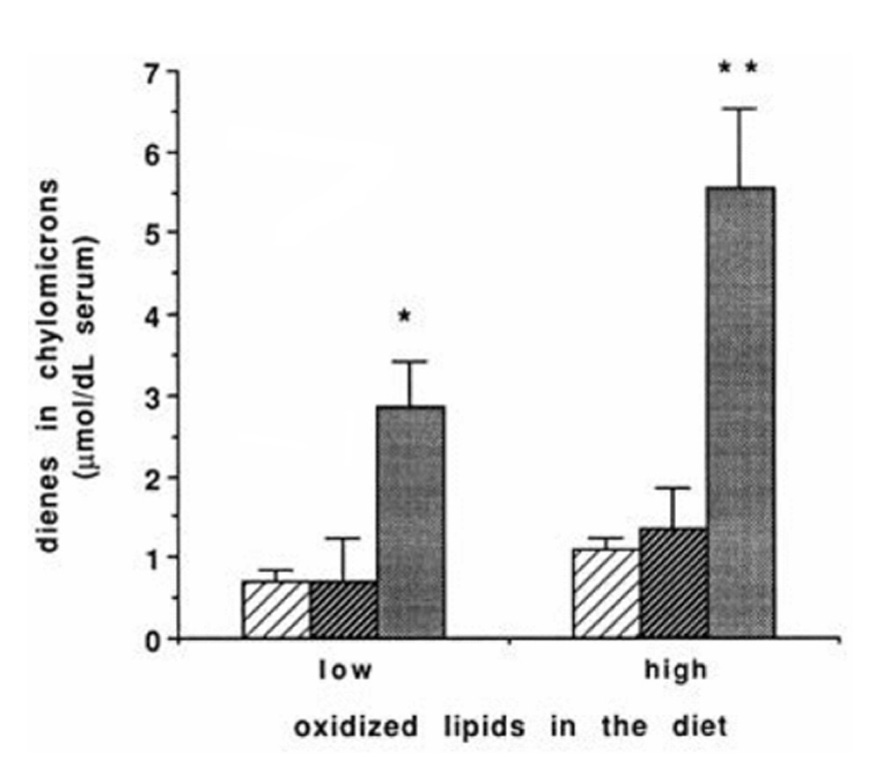
Ewwww, that doesn't look good, does it? But here are two graphs from the same study, which Mason did not feature in his presentation, that show how oxidised dietary cholesterol remains in the bloodstream of healthy human subjects for three days, and is incorporated into their circulating lipoproteins:
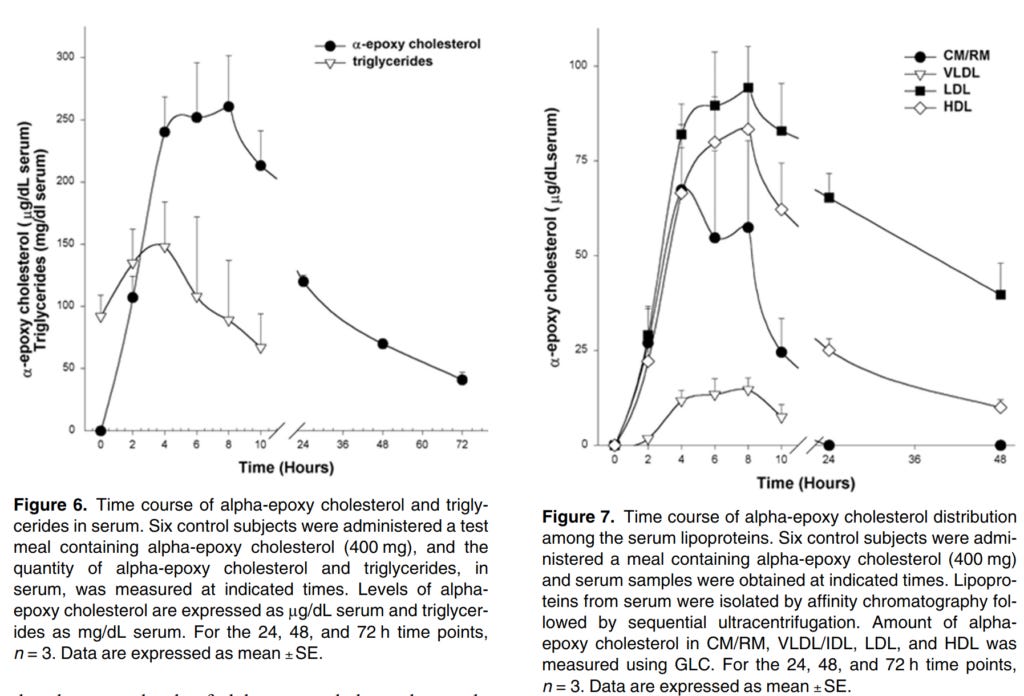
If Mason is as deeply concerned about the impact of oxidation products in the blood on atherosclerotic cardiovascular disease as he purports to be, why didn't he sound the alarm about oxidised cholesterol, which is formed when animal-sourced food products are heated (especially in dry heat processes)? After all, oxidised cholesterol elevates oxidation products in the bloodstream of healthy people for as long as oxidised fats persisted in the blood of poorly-controlled diabetics.
Finally, it's important to point out that Mason's claim that "thrombosis... is the source of atherosclerosis" has not been proven by any of the evidence he presents in this talk. Thrombosis is one of many contributing causes of the atherosclerotic process, and it turns out that elevated LDL-cholesterol, and to an even greater extent apolipoprotein B, are causally involved in many, if not all, of these processes.
Whew, two solid days of researching and writing, and I'm still only one third of the way through this video! If you appreciate my work, and would like to support me to do more in-depth critiques like this one, please consider a paid subscription to my Substack.
N.B. I’ve now completed my appraisal of Dr Paul Mason’s presentation, which you can read here:

For information on my private practice, please visit Empower Total Health. I am a Certified Lifestyle Medicine Practitioner, with an ND, GDCouns, BHSc(Hons) and Fellowship of the Australasian Society of Lifestyle Medicine.
It's important to acknowledge that there are major controversies about the benefits and risks of statins. As one of my favourite websites for appraising the risk:benefit ratio of medical interventions, The NNT, puts it:
"Virtually all of the major statin studies were paid for and conducted by their respective pharmaceutical company. A long history of misrepresentation of data and occasionally fraudulent reporting of data suggests that these results are often much more optimistic than subsequent data produced by researchers and parties that do not have a financial stake in the results."
Statins Given for 5 Years for Heart Disease Prevention (With Known Heart Disease)
Nonetheless, the failure of the authors of this systematic review to make any attempt to appraise the potential for confounding resulting from participants commencing lipid-lowering treatments after study enrolment, is a major methodological error.
Excellent article. Humans are omnivores. Trying to convert the human body to that of a carnivore is like trying to turn your dog into a vegan. Bad news.
I'm looking forward to the rest of your research. Thank you.