


Australia’s drug regulator is leading the race to the bottom
... surprising pretty much no one.

Over the past two and a half years of covidiacy, we have witnessed institutional failure on a truly epic scale. From the news media, to scientific and medical journals, universities and schools, unions (including those representing health professionals and teachers), regulatory bodies – practically every institution that we should have been able to rely upon to contest the official narrative, offer and robustly debate alternative explanations and solutions, and hold policy-makers’ feet to the fire, has instead obsequiously echoed every absurd official talking point like so many parrots in a cage.
Of all these institutions, the failure of medical journals and of national drug regulators to do their respective jobs properly has been among the most visible, and perhaps the most consequential.
A drug regulator’s job is to ensure that only new products with a balance of safety and effectiveness appropriate to the disease they’re intended to treat, reach the market. We’ll come back to how they’ve performed, a bit later.
The role of medical journals is to provide a forum for the robust debate of competing hypotheses that the entire scientific enterprise depends on, while also ensuring quality control through the process of stringent review of emerging findings by appropriately-qualified peers. How have they done?
Well, who can forget the Lancet – one of the oldest and most respected medical journals in the world – publishing a letter branding anyone who questioned the fanciful ‘a bat had a tryst with a pangolin in a wet market and hey-presto, a perfectly human-adapted coronavirus emerged, just like that!’ official origin story of SARS-CoV-2 as a racist conspiracy theorist… and then admitting with embarrassment, after US Right to Know obtained emails relating to the Lancet letter, that said letter was authored by Peter Daszak, the head of EcoHealth Alliance. You know, the organisation which had received millions in US taxpayer-funded grant money to carry out dangerous gain-of-function research on coronaviruses at the Wuhan Institute of Virology? That Peter Daszak.
In the mean time, Lancet had appointed the same individual to its commission to investigate the origins of the virus, only to have to recuse him and shut down the origins investigation once the stench of Daszak’s blatant conflicts of interest became too high even for its well-seasoned nostrils:
Lancet continued to cover itself in glory by publishing a study which purported to find that COVID-19 patients treated with chloroquine or hydroxychloroquine had a higher risk of dying, only to retract it barely two weeks later when independent doctors, researchers and the few journalists still worthy of that title discovered that the dataset on which the study was based was completely fabricated.
The company which supplied the purportedly global dataset of hospital admissions, Surgisphere, comprised a handful of part-time staff members including a science fiction author/fantasy artist, and an adult model/events hostess. (I covered this bizarre instalment of ‘This Week in Covidiacy’ in The strange tale of hydroxychloroquine.) Apparently the Lancet’s vigorous peer review process was not capable of discovering the fraud, while a bunch of dudes on Twitter were.
The New England Journal of Medicine, another top-ranked medical journal, also blundered into the Surgisphere snare. Its article reassuring doctors that COVID-19 patients were not adversely affected by taking blood pressure drugs that act on the ACE receptor was also retracted, seven days after publication, when the itty-bitty-teeny-weeny completely fake database problem was exposed.
Meanwhile, it’s increasingly difficult to distinguish the Journal of the American Medical Association from the Babylon Bee. JAMA devotes ungodly amounts of page space to pressing issues like the appropriate use of inclusive language by health care providers (that’s a chestfeeding birthing person, not a breastfeeding mother, you bigoted oppressor) and how to achieve complete racial, ethnic and gender/transgender parity in every medical speciality.
(Personally, I don’t give a crap what percentage victim my health care providers are, as long as they can damn well do their jobs without the government’s attack dog, AHPRA, gagging and threatening to deregister them if they question any of the completely non-evidence-based public health policies.)
Then there are the narrative-bucking studies that did manage to pass peer review and get published, and were then retracted (most often violating the accepted processes for doing so) when medical journals came under fire for having the temerity to give a platform to anyone who hadn't drunk the Kool-Aid.
Harald Walach's paper demonstrating that levels of carbon dioxide in inhaled air in children wearing face masks exceeded those deemed unacceptable by the German Federal Environmental Office1; Ronald Kostoff's analysis finding five times the number of deaths attributable to each COVID-19 injection vs those attributable to COVID-19 itself in the most vulnerable 65+ demographic2; and Jessica Rose and Peter McCullough's study finding a markedly higher risk for myocarditis associated with COVID-19 injections than for other known vaccines3, are just three examples of this dangerous trend.
The one small, faintly flickering lighthouse in this ocean of mediocrity has been the British Medical Journal, which, in this age of the acronym, now goes by the much-snappier BMJ.
While certainly publishing its fair share of experimental injection cheerleading and ideologically-motivated twaddle (like this choice piece in which the editor in chief blasted two recent US Supreme Court decisions for their purported effects on ‘public health’, without any evident awareness of his own total gormlessness in wading into constitutional arguments that have occupied legal minds far more brilliant than his for decades), the BMJ has, to its credit, thrown its institutional weight behind prominent dissenters from the COVID orthodoxy.
It was the BMJ that commissioned and published Paul Thacker’s stunning investigation of poor research practices and data integrity issues in the pivotal Phase 3 trial of the experimental Pfizer COVID-19 injection, which I discussed in my previous article “Safe and effective” – because Pfizer says so! The allegations made by Thacker’s main whistleblower, Brook Jackson, are currently the subject of a fraud lawsuit.
And the BMJ has courageously backed its senior editor, Peter Doshi, PhD (who is also Associate Professor of Pharmaceutical Health Services Research at the University of Maryland) in penning a series of editorials criticising the design of the clinical trials of the experimental COVID-19 injections for omitting the endpoints that actually mattered, castigating drug regulators for rushing headlong into granting full approval of the injections despite insufficient safety and efficacy data, calling out the media’s incessant use of COVID dashboards for delaying the return to normal social and economic life, and blasting pharma companies for refusing to release data on their COVID-19 injections and drugs.
Now, BMJ continues its proud tradition of supporting independent medical journalism on issues that actually matter, with its publication of an investigative piece on the funding, conflicts of interest, and performance of international drug regulating bodies. The article, From FDA to MHRA: are drug regulators for hire?, was authored by Maryanne Demasi.
Australian readers will remember Demasi for two separate firestorms of controversy that she ignited as a medical reporter on the ABC’s flagship science program, Catalyst. The 2013 episode questioning the value of statins provoked that pharma favourite, Aunty’s Dr Norman Swan (whose bio indicates he hasn’t actually treated a patient for four decades) into paroxysms of panic-porn over the deaths that were sure to result if people – especially the Indigenous for whom he apparently cares so deeply – stopped taking their life-saving statins.
(Side note: statins show no benefit in saving lives from heart disease in people with no cardiovascular disease history [i.e. primary prevention], and no mortality benefit in people at low risk of cardiovascular disease. Among people with known heart disease, 83 would have to take a daily dose for five years to save one life from a cardiovascular cause, during which one in fifty will develop diabetes and one in 10 will suffer muscle damage. Sounds like a sweet deal.)
Then in 2016, Demasi was suspended by the ABC over her story on potential dangers of wireless devices such as mobile phones. The fact that the International Agency for Research on Cancer of the World Health Organisation (which we’re supposed to accept as the ultimate arbiter of health truthiness when they opine on anything else) had classified radiofrequency electromagnetic fields such as those emitted by mobile phones as a Group 2B carcinogen – that is, possibly cancer-causing in humans – in 2011 mattered not. Demasi had offended the telecomms industry gods, and a suitable penance had to be exacted in order to appease them.
Fortunately, Demasi was not chastened by her experiences at Australia’s publicly-funded broadcaster/industry lapdog, and has gone on to much greener pastures as an independent investigative journalist.

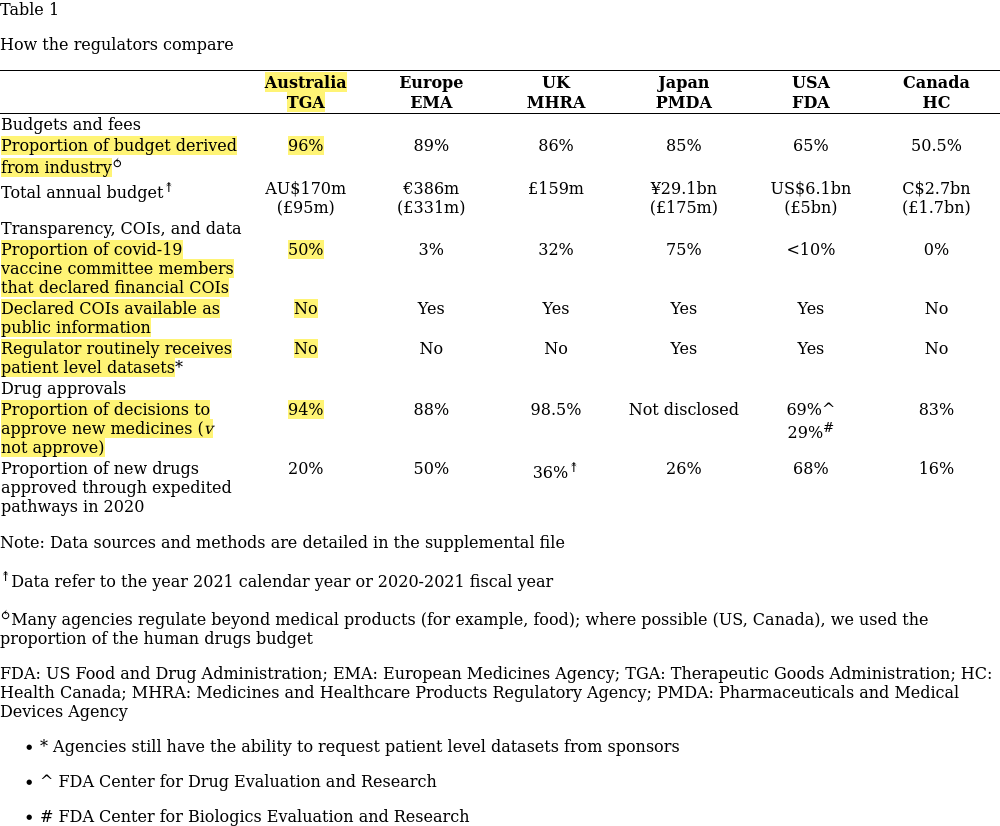
BMJ commissioned Demasi to investigate six national/transnational drug regulatory agencies: Australia’s Therapeutic Goods Administration (TGA), the European Medicines Agency (EMA), the UK’s Medicines and Healthcare Products Regulatory Agency (MHRA), Japan’s Pharmaceuticals and Medical Devices Agency (PMDA), the US Food and Drug Administration (FDA) and Health Canada (HC).
If her findings don’t cause you to sleep uneasily tonight, you’re clearly not paying attention. The summary table tells the tale; I’ve highlighted the most eye-popping facts for my Australian readers.
Let’s go through these key findings one by one, again with a focus on TGA.
1. 96 per cent of TGA’s budget comes from industry fees
TGA’s closest rival for ‘most compromised drug regulatory agency investigated’ was the EMA, which garners 89 per cent of its budget from the industry it’s supposed to be guarding. In contrast, the much-maligned FDA only gets 65 per cent of its funding from industry user fees, while Health Canada did best at just a smidgen over 50 per cent.
If the fact that Australia’s national drug regulator draws practically its entire operating budget from fees paid by drug and device manufacturers doesn’t prompt you to ask “Could TGA be a captured agency?”, it’s possible that a) you forgot to plug in your brain when you woke up this morning or b) you’re from the TGA itself4, which responded to Demasi’s probing by “firmly den[ying] that its almost exclusive reliance on pharmaceutical industry funding is a conflict of interest (COI).” Demasi goes on,
“In response to a query, the agency said, ‘All fees and charges are prescribed in our legislation. To provide transparency, the TGA fees and charges are published on the TGA website.’”
Well, that clears that up, doesn’t it? I mean, your new girlfriend couldn’t possibly be a hooker if she told you up-front how much she charges, could she? Move along, nothing to see here.
2. Five out of ten members of the TGA committee that decides which vaccines will be used in Australia admit to conflicts of interest with the vaccine industry
Demasi’s findings on conflicts of interest in TGA’s Advisory Committee on Vaccines, whose ambit is “issues relating to pre-market assessment, post-market monitoring and safe use in national immunisation programs”, are so shocking, they are worth quoting at length:
“In Australia, the membership of the TGA’s Advisory Committee on Vaccines is published on the agency’s website. The forms for recording past and current financial and non-financial interests are not, however, made public. A Freedom of Information (FOI) Act request for their financial disclosures in August 2020 had names and details of the disclosures redacted.13 After seeking additional details, the TGA indicated that this was ‘personal information’ and therefore usually exempt under the FOI act. Subsequently, panel members were approached directly by email and asked whether they would be willing to publish their declarations, but there was no response. Instead, they referred the enquiry back to the TGA which was willing to reveal that 5 of 10 committee members disclosed COIs—but did not say which members or provide any specifics, adding that ‘these interests usually do not give rise to a conflict.’ The agency’s policy allows for excluding members from certain meetings because of a COI, but details of the COI and reasons for the exclusion are not published.”
You think you’re entitled to know which committee members have been wined, dined and sixty-nined by the vaccine manufacturers who stand to make a liability-free killing if their product gets onto the national vaccine schedule? Shut up and keep paying your taxes, peon; that’s not for you to know. The smart people have decided that, as a for instance, having received money or gifts from an industry or being offered a lucrative corporate job or consultancy doesn’t influence committee members’ decision-making. “Usually.”
Only Japan’s drug regulator was more obviously compromised, with three quarters of vaccine committee members declaring a conflict of interest, compared to only 3 per cent of Europe’s and none of Canada’s. And Canada is the only other country covered in Demasi’s analysis which doesn’t make such disclosures public knowledge.
3. TGA does not routinely undertake its own assessment of clinical trials used to obtain product approval, but instead relies on summaries of these trials provided by drug companies
In fact, only the US and Japanese drug regulators routinely undertake patient-level analysis of the clinical trials that are designed, conducted, analysed and reported by the companies seeking regulatory approval for their drugs, biological products and devices.
For those of you deluded enough to believe that TGA’s assurance that it “will rigorously assess any COVID-19 vaccine for safety, quality and effectiveness” means that its committee members are poring through reams of data, demanding to know, for example, why Brianne Dressen’s catastrophic injury was air-brushed out of the AstraZeneca trial results, or how Pfizer managed to classify teenager Maddie de Garay’s life-altering reaction to its experimental product, which has left her paralysed from the waist down, incontinent, in constant full-body pain and reliant for nutrition on a nasogastric tube, as “functional abdominal pain”, it’s time to wake up and smell the self interest:
“The TGA… says it conducts its covid-19 vaccine assessments based on ‘the information provided by the vaccine’s sponsor.’ According to a FOI request from last May, the TGA said it had not seen the source data from the covid-19 vaccine trials. Rather, the agency evaluated the manufacturer’s ‘aggregate or pooled data.’ The TGA does not have the individual participant level datasets pertaining to the covid-19 vaccine trials,17 which are held by the vaccine manufacturer.”
In other words, TGA doesn’t even put the drug and vaccine industry to the bother of having to invoke the ‘dog ate my homework’ excuse. Pharma companies can just cross their hearts and promise the regulator that they really, truly, honestly did do their homework… and the TGA believes them. And on the basis of this highly rigorous process…
4. TGA approves 94 per cent of new medicines
Only the MHRA has a lower bar, unleashing 98.5 per cent of medicines that cross its regulatory desk onto the unsuspecting UK public. In contrast, FDA approved just 67 per cent of drugs and 29 per cent of biologics.
One wonders just how outrageously inadequate a drug, device or biologic sponsor’s application has to be for this industry lapdog to knock it back. Actually, flicking through TGA’s Recalls gives clues. Granny developed heart problems from her TGA-approved Alzeimer’s drug? Oopsie. TGA-approved shingles vaccine gave you infectious chickenpox? Sorry about that, Chief. Got dangerously addicted to your TGA-approved pain meds? Our bad.
The only thing TGA isn’t doing worse than practically all of the other regulators is rushing drugs through an expedited approvals pathway (read: even laxer than usual standards). Only 20 per cent of pharmaceutical products that gained TGA approval in the period Demasi examined (2021 calendar year or 2020-2021 fiscal year) had proceeded through an accelerated approval process, compared to half of EMA’s approvals and 68 per cent of FDA’s.
On the other hand, when 94 per cent of applications get rubber-stamped by TGA anyway, why would drug companies bother stumping up extra money to get a fast-tracked approval?
Are drug regulators too far gone to reform?
Demasi asked several medical academics how they would solve the problems her investigation had identified. Most proposed structural reforms ranging from minor to sweeping, but sociologist Donald Light of New Jersey’s Rowan University expressed zero confidence that any such measures would be sufficient to restore these toothless lapdogs to their purported role as fierce watchdogs over an industry with a long and rich history of corporate criminality.
Light told Demasi,
“It’s the opposite of having a trustworthy organisation independently and rigorously assessing medicines. They’re not rigorous, they’re not independent, they are selective, and they withhold data. Doctors and patients must appreciate how deeply and extensively drug regulators can’t be trusted so long as they are captured by industry funding.”
Instead, Light proposed “setting up non-profit organisations like Germany’s Institute for Quality and Efficiency in Health Care, which was established to carry out evaluations of approved drugs that are independent of industry, rigorous, unbiased, and transparent.” You know, like the regulators were supposed to be. But aren’t.
Take-home lessons for the public
Drug regulatory agencies are textbook examples of regulatory capture, long since co-opted to not disrupt the commercial, ideological and political interests of the serially criminal industry they are supposed to police on behalf of the public.
Governments don’t care, because prostituting regulatory agencies to the industry they’re supposed to regulate through the imposition of ‘user fees’ frees them up to spend your tax dollars on all manner of other boondoggles that increase their chances of re-election.
Most doctors rely on national regulators to do the job of drug, biologic and device safety assessment for them. The vast majority of prescribers assume that “FDA/TGA/MHRA-approved” means “as safe as mother’s milk”, and never bother reading, let alone critically analysing, any of the clinical trial data that garnered these products’ approval. Let’s face it, would any health practitioner who had actually read the Supplementary Appendix to Pfizer’s six month safety and efficacy study and discovered that more people who took the Pfizer COVID-19 jab than the placebo died in the course of the study have injected this stuff into any of their patients?
Most medical journals are also deeply corrupted by the same process of regulatory capture, as has been acknowledged by industry insiders including former New England Journal of Medicine Editor-in-Chief Marcia Angell, who wrote in 2009 that “it is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines”. Long-time Lancet editor Richard Horton similarly opined in 2015, “The case against science is straightforward: much of the scientific literature, perhaps half, may simply be untrue. Afflicted by studies with small sample sizes, tiny effects, invalid exploratory analyses, and flagrant conflicts of interest, together with an obsession for pursuing fashionable trends of dubious importance, science has taken a turn towards darkness.” … And then he piloted his journal full steam into said darkness as soon as the scamdemic hit. Who wants to be a prophet in his own land, anyway?
The safest drug to take is no drug at all and the next safest is one that’s been in widespread use for at least 20 years. Better yet, why not start taking responsibility for your own health and getting off those darn drugs, already?
For information on my private practice, please visit Empower Total Health. I am a Certified Lifestyle Medicine Practitioner, with an ND, GDCouns, BHSc(Hons) and Fellowship of the Australasian Society of Lifestyle Medicine.
Not necessarily mutually exclusive with a).
Love this work, the plain truth of the level of Criminality is overwhelming, with the likes of Peter Daszak,
whose infamous statement, " the profit will follow the hype" is of itself, a true indication of the contempt, and the irrational conduct, its nothing personal, its just business, of these corrupt creatures.
With, the ye olde school tie cronies of the closed shop TGA, who like the bootleggers of ATAGI, are answerable to no- one, just performing as another financial cog in the wheel of gratuitous , " it us, not them" crowd, whose blatant, negligence and failure of any semblance of Duty of Care is breathtaking,
as is the belligerent AHPRA, Whose thuggery, and tyrannical behaviour, is a blight on this Country.
Brilliant work, enjoy your writing style , down to earth:
Thank you for your wonderful common sense. Why not take control over our health rather than wishing for a quick fix when there are no magic bullets.
Thank you for all your research,
Annette