Positive psychology researchers - not to mention philosophers and religious sages - tell us that consciously cultivating gratitude is one of the best ways to enhance happiness. Well, here's one thing I'm grateful for: my wonderful readers, who often provide me with topics for my posts, and whose thoughtful comments frequently stimulate me to think more deeply, work on expressing myself more clearly, and delve into avenues of research that I otherwise wouldn't bother with.
I'm sure TheLastBattleStation isn't alone in experiencing this sense of frustration with the endless to-ing and fro-ing over nutrition advice. I've encountered many people, both in my personal and professional life, who have simply switched off. They just don't pay any attention to the pronouncements of 'experts' on nutrition; instead, they either eat whatever they enjoy, or they employ a simple heuristic such as "If my grandmother ate it, it's probably healthy." I have complete sympathy for people who adopt either of these approaches. As TheLastBattleStation expressed it, how can two people, or two groups look at the exact same data and draw two opposite conclusions?... and if these competing groups can't agree on the interpretation of basic data, why should the average person pay attention to them at all?
However, as I've discussed previously, the general public's impression that various camps within the world of nutrition research hold radically different viewpoints on what constitutes a healthy diet, is largely a false perception generated by the online spectacles that power the attention economy of social media. Twitter flame wars, Instagram pile-ons, and hyperbolic YouTube thumbnails will always attract infinitely more audience attention than serious scholarly debates, but in point of fact, the vast majority of professionals who have devoted their lives to investigating the role of nutrition in human health and disease actually agree on far more than they disagree on. As I wrote in Debunking nutrition myths: A how-to guide,
"Would you be surprised to learn that plant-based diet advocates such as Emeritus Professor T. Colin Campbell and Dr Dean Ornish are in fundamental agreement on human nutrition with paleo diet advocates such as Professor Emeritus Loren Cordain and Dr Boyd Eaton? Well, they are. That’s why all four are THI [True Health Initiative] Council Members. So if you are going to follow the siren song of the self-appointed nutrition gurus who claim that all the nutrition experts are wrong about what constitutes a healthy diet for humans, you won’t have much left to eat."
To address TheLastBattleStation's specific statements and questions, I need to provide a little more background on cholesterol metabolism and transport than I did in last week's post. For openers, let's recap the basics:
"Cholesterol is a fatty, waxy substance which is found in all animal cells, both as a structural component of cell membranes, and a cell signalling molecule. It’s also a precursor for the synthesis of steroid hormones including so-called ‘vitamin D’, testosterone, oestrogen and cortisol; and for bile acids, which are necessary for fat digestion and absorption of fat-soluble nutrients.
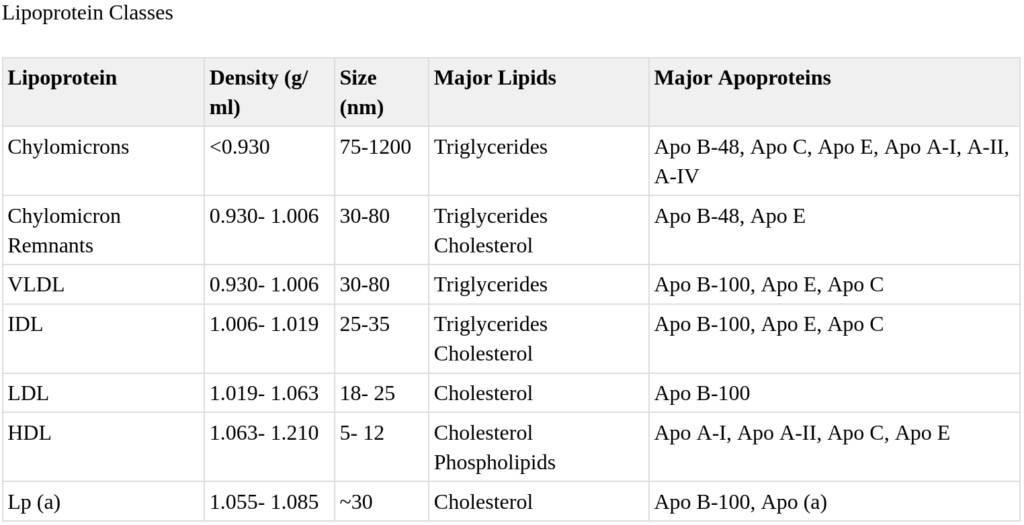
Notoriously, oils or fats and water don't mix. So in order for triglycerides - the most common form of fat in the body - and cholesterol - also a fatty/waxy substance - to be able to travel throughout the body via the watery medium of the blood plasma, they must be packaged up in lipoproteins which are, as the name implies, molecules that comprise both fats (lipids) and proteins. There are seven classes of plasma lipoproteins, differentiated by their density, size, lipid composition, and which type/s of apolipoproteins (proteins that bind and transport lipids) they contain.
As they travel around the body, picking up fats and cholesterol from various locations and setting them down in others, lipoproteins transform from one class to another, to another:
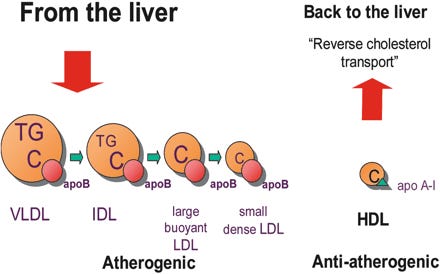
Figure 1: There is only one apoB in each particle of VLDL, IDL, large buoyant, and sd-LDL. Thus, the total apoB represents the total number of potentially atherogenic particles. ApoA-I is the main protein in HDL particles and is responsible for the initiation of the ‘reverse cholesterol transport’. The balance between apoB and apoA-I, i.e. the apoB/apoA-I ratio, indicates cardiovascular risk; the higher the ratio, the higher the risk. From Rationale for using apolipoprotein B and apolipoprotein A-I as indicators of cardiac risk and as targets for lipid-lowering therapy.
For our current purposes, we primarily need to consider low-density lipoprotein cholesterol (LDL-C) and high-density lipoprotein cholesterol (HDL-C). Educational material written for public consumption (and even for health professionals) often dumbs down the description of these two important lipoproteins to 'bad cholesterol' and 'good cholesterol' respectively, conveying the false impression that there are two distinct types of cholesterol. This is nonsense - and unfortunately, it's nonsense that feeds the online trolls who promote the fable that LDL-C levels have nothing to do with atherosclerotic cardiovascular disease. Cholesterol is cholesterol is cholesterol; it's neither bad, nor good.
Instead, the key difference between LDL-C and HDL-C is that LDL-C contains apolipoprotein B-100 (apo B-100, usually abbreviated simply to apo B), which can initiate atherogenesis - the build-up of atherosclerotic plaque in the inner lining of blood vessels - whereas the latter contains apolipoprotein A-1, which facilitates reverse cholesterol transport, or the trafficking of cholesterol from various sites throughout the body to the liver, which processes cholesterol for elimination.
But what specific circumstances cause LDL-C, and its payload of apo B, to initiate atherogenesis? Quite simply, when there's too much of it. Remember, apolipoproteins are molecules whose purpose in life is to transport lipids (including cholesterol) around the body, and to deliver those lipids to cells. Apo B is recognised by LDL receptors found on the surface of many of the body's cells - including those that line our arteries. Specifically, apo B has a high affinity for binding proteoglycans- protein compounds found in artery walls. And so, even in the absence of additional risk factors such as oxidative stress and inflammation, excessive apo B drives atherosclerosis by causing lipoproteins to become entrapped in the arterial wall. And in fact, small dense LDL particles, which contain the lowest ratio of cholesterol to apoB, "are the most atherogenic particles because they are easily oxidized and promote an inflammatory response and the growth of plaques". That is to say, once apo B has driven LDL-C (especially the small dense type) and other apo B-bearing lipoproteins into the delicate lining of an artery, immune cells react by mounting a defensive response (inflammation and oxidation) that ends up initiating a plaque.
And now we get to the $64 000 question, which underlies TheLastBattleStation's cynicism about contradictory nutrition claims: What causes levels of LDL-C, and hence of apo B, to rise so high that they initiate atherosclerosis? It's not dietary cholesterol, as TheLastBattleStation correctly noted. Serum cholesterol rises linearly with increasing dietary cholesterol intake up to a daily intake of 300-400 mg of cholesterol. Above this, the dose-response curve becomes hyperbolic. What this means is that if you start feeding cholesterol to vegans, you'll see their serum cholesterol steadily rise with each increment of increase in dietary cholesterol, but once they go beyond the amount that's contained in a couple of eggs, or a bacon, egg and cheese McMuffin and a cup of cooked chicken, there's very little further increase in serum cholesterol. The egg industry has exploited this fact by designing studies that demonstrate that adding one or more eggs per day to the standard American diet causes little clinically meaningful change to participants' cholesterol levels.
Instead of dietary cholesterol, the major dietary factor that raises serum total and LDL-cholesterol, and apo B is - drumroll please - saturated fat.
Saturated fat, which is characterised by being solid at room temperature (think butter, ghee, lard, tallow, coconut oil and palm oil) has been known to be the major dietary component that raises LDL-C levels, since Hegsted published the results of his extensive experiments on the effect of 36 different types of oils and fats on serum cholesterol, in 1965. Since then, the impact of saturated fat intake on LDL-C and apo B has been extensively documented. For example:
A quantitative meta-analysis of metabolic ward studies concluded that replacing just 10 per cent of calories from saturated fat with an equivalent calorie amount of complex carbohydrates, would reduce LDL-C by 0.36 mmol/L (14 mg/dl).
Dropping saturated fat intake from 15 per cent of daily calories to 6 per cent for 8 weeks, decreased participants' LDL-C by almost twelve per cent, by upregulating the number of LDL-receptors, which clear LDL-C from the body.
In Pima Indians (well known for their tragic susceptibility to developing type 2 diabetes), when saturated fat intake was reduced from 21 per cent of daily calories to just 6 per cent, LDL-C dropped by around 16 per cent in nondiabetics and diabetics alike, while LDL apoB fell by 13 per cent.
To concisely summarise that body of evidence, there is a clear dose-response relationship between serum levels of LDL-C/apo B and the risk of atherosclerotic cardiovascular disease-related events such as heart attacks, strokes, coronary revascularisation procedures and cardiovascular death. Whether you have a lower LDL-C/apo B because you won the genetic lottery, or because you follow a diet and/or exercise regimen or use medications or supplements that reduce your LDL-C/apo B, it's all the same: lower LDL-C/apo B = lower risk of atherosclerotic cardiovascular disease.
Thanks for reading Empowered! This post is public so feel free to share it.
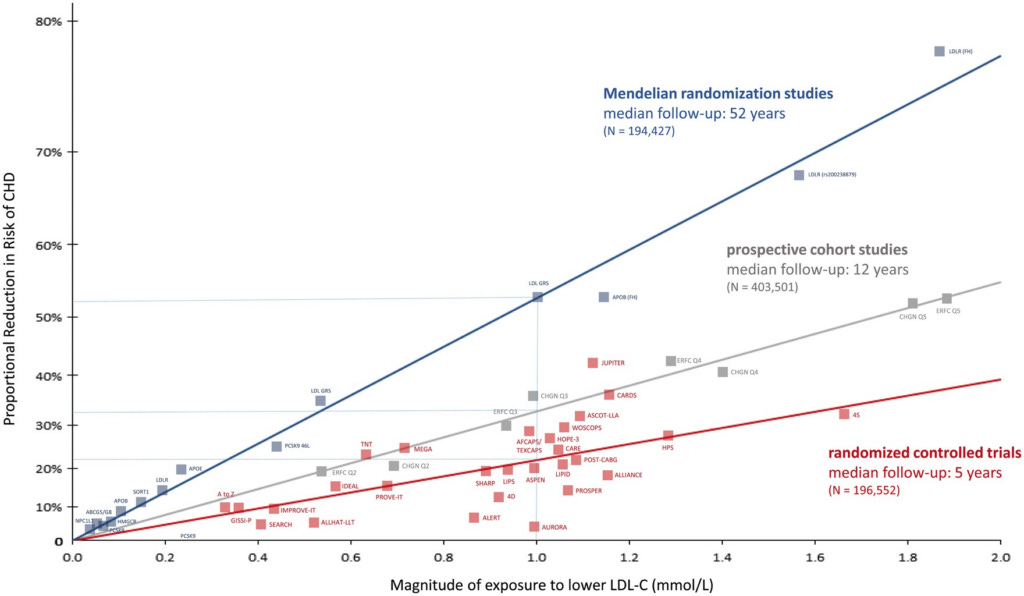
However, there is a cumulative effect of having a lower LDL-C/apo B; that is, the more years of your life that you've lived with low LDL-C, the greater will be your reduction in risk. Conversely, if you've lived for 50-60 years with the unnaturally high total and LDL-C typically seen in populations eating Westernised diets, and then start taking a statin after you've already developed atherosclerosis, you won't get as much benefit. The following figure clearly illustrates this cumulative effect. The Mendelian randomisation studies (which reflect lifelong exposure to low LDL-C levels due to favourable gene variants) show up to nearly 80 per cent reduction in risk of coronary heart disease in people with 1.9 mmol/L lower LDL-C, whereas the most impressive reduction in risk achieved by a cholesterol-lowering medication was only 40 per cent:
Figure 2: Log-linear association per unit change in low-density lipoprotein cholesterol (LDL-C) and the risk of cardiovascular disease as reported in meta-analyses of Mendelian randomization studies, prospective epidemiologic cohort studies, and randomized trials. The increasingly steeper slope of the log-linear association with increasing length of follow-up time implies that LDL-C has both a causal and a cumulative effect on the risk of cardiovascular disease. The proportional risk reduction (y axis) is calculated as 1−relative risk (as estimated by the odds ratio in Mendelian randomization studies, or the hazard ration in the prospective epidemiologic studies and randomized trials) on the log scale, then exponentiated and converted to a percentage. From Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel
I have never seen a persuasive rebuttal of this large body of evidence by any of the critics of the lipid-heart hypothesis and god only knows, I've read plenty of them and comprehensively debunked quiteafew.
What does 'higher' and 'lower' actually mean?
If you, like TheLastBattleStation, are feeling frustrated by my use of vague terms like 'higher' and 'lower', I feel ya. There are such substantial differences between individuals in every aspect of cholesterol and lipoprotein metabolism, and in the prevalence of other risk factors for cardiovascular disease such as high blood pressure and insulin resistance, that it's not possible to stipulate the exact LDL-C or apo B level that would optimally reduce the risk of atherosclerotic cardiovascular disease in any given individual. However, as Loren Cordain and co-authors pointed out in the 2004 paper that I cited in last week's post,
"The normal low-density lipoprotein (LDL) cholesterol range is 50 to 70 mg/dl for native hunter-gatherers, healthy human neonates, free-living primates, and other wild mammals (all of whom do not develop atherosclerosis). Randomized trial data suggest atherosclerosis progression and coronary heart disease events are minimized when LDL is lowered to <70 mg/dl. No major safety concerns have surfaced in studies that lowered LDL to this range of 50 to 70 mg/dl."
N.B.: 50 mg/dl is 1.3 mmol/L, and 70 mg/dl is 1.8 mmol/L.
The authors of a more recent review published in 2022 suggested that optimal LDL-C may be even lower, although fortunately it may not be necessary to achieve this optimum for clinical benefit:
"Normal LDL-C is 20–40 mg/dL
Humans were never meant to harbor the low-density lipoprotein cholesterol (LDL-C) levels that are now commonplace. In one series of 147 full-term neonates, the average LDL-C was 20 ± 10 mg/dL [59] Despite the extraordinary rate of development and need for myelination, even neonates need very little LDL-C [60], [61], [62], [63]. The fact that animals, non-human primates, and humans who maintain low cholesterol levels from early in life have very little atherosclerosis all suggest that a ‘normal’ non-atherogenic LDL-C level is 20–40 mg/dl. That is of course difficult to achieve in a modern society and, as described herein, is not necessary for most people.
Based on the log-linear relationship of LDL-C to the hazard ratio for an acute ASCVD event, the LDL-C level where no excess risk occurs is approximately 38 mg/dL or 1 mmol/L [64] (Fig. 1). This value is consistent with the LDL-C levels observed among hunter-gatherer populations [65,66]. In the Framingham Study, the average LDL-C of a man presenting with an Acute Coronary Syndrome (ACS) is approximately 150 mg/dL [67]. In the Cooper Center Longitudinal Study, even when LDL-C at baseline was < 100 mg/dL, there was a continuous rise in risk for Coronary Heart Disease (CHD) mortality over a mean follow-up time of 26.5 yrs [68,69] Hence, it is crucial that exposure to atherogenic lipoproteins be dramatically reduced early and over the long-term.
Now, I don't know whether the cholesterol numbers that TheLastBattleStation cited in his comment were total or LDL-C, but I presume they were the former. The ratio between total and LDL-C varies between individuals, but Cordain et al state that a total cholesterol of 140 mg/dl corresponds to LDL-C of approximately 70 mg/dl. Therefore at TheLastBattleStation's highest measured (presumed) total cholesterol of 170 mg/dl, his LDL-C would have been approximately 85 mg/dl - still relatively low risk, but starting to creep up.
Get more from Robyn Chuter in the Substack app
Available for iOS and Android
That's all very well; now what do I do?
To assess your current level of cardiovascular risk and decide whether it requires action, I recommend seeing your GP to request a blood test for apolipoprotein B. If it is higher than 100 mg/dl (1 g/L in Australian measures), or above 80 mg/dl (0.8 g/L) if you're at very high cardiovascular risk, my advice would be to undertake a comprehensive diet and lifestyle program aimed at reducing apo B/LDL-C and overall cardiovascular risk. This program may include some or all of the following:
A diet very low in trans fats, saturated fat, refined carbohydrates and dietary cholesterol (particularly if you're a cholesterol hyperabsorber, which you can assess by testing for sitosterol, campesterol, and/or cholestanol), and high in fibre and omega-3 fats - essentially, a plant-centric diet possibly augmented with oily fish (preferably very small ones, to minimise the toxic contamination issue);
Finally, I want to address TheLastBattleStation's comment regarding statistics:
"My opinion is that all the numbers we are given as to what is healthy are just that - numbers. Statistics."
Obviously, this is true. Scientists calculate statistical probabilities based on large datasets. These probabilities apply to groups with particular characteristics, not to individuals within those groups. No researcher or clinician can tell you your exact risk of developing cardiovascular disease, or any other condition, nor can they tell you the exact percentage by which you will reduce your risk if you undertake any individual therapy, or combination of them. If you want certainty about any of these matters, it looks like you picked the wrong planet!
As far as I can see, our best chance of enjoying a long, healthy life with minimal risk of atherosclerotic cardiovascular disease, is to heed the vast body of research that I've outlined in this post (and previousones). But I can't compel you to do so, and I wouldn't even if it were possible, because I respect your autonomy. You're an adult, you can read, and you can train yourself, if you choose to do so, to assess evidence and decide for yourself whether it's reliable and worth actioning, or not. Over to you.
And finally, this post has taken me approximately 15 hours to research and write. Sifting through endless studies and extracting the nuggets of actionable information is an arduous business! I make all my posts freely available to all readers, because I believe we all deserve access to information that helps us to take greater control over our health. But I rely on my small core of paid subscribers to provide this service to those who genuinely can’t afford it.
Empowered! is a reader-supported publication. Without the generous support of my paid subscribers, I could not continue to bring you this important information.
For information on my private practice, please visit Empower Total Health. I am a Certified Lifestyle Medicine Practitioner, with an ND, GDCouns, BHSc(Hons) and Fellowship of the Australasian Society of Lifestyle Medicine.
Have you heard of Dr. Malcolm Kendrick? A Scottish doctor and author of The Cholesterol Con and A Statin Nation. If your research had included this doctor your conclusions might have been different.







Have you heard of Dr. Malcolm Kendrick? A Scottish doctor and author of The Cholesterol Con and A Statin Nation. If your research had included this doctor your conclusions might have been different.