


The vitamin D-ilemma Part 4
Does low vitamin D cause disease, or does disease cause low vitamin D?

Part 4: Reverse causation - cart before horse?
In Part 3 of this miniseries, I discussed the disconnect between the outcomes of observational studies which found an association between low 25-hydroxyvitamin D levels and a dizzying array of diseases, and clinical trials which found that supplementation with vitamin D did not prevent or alleviate most of those conditions.
The discordance between these two types of evidence ultimately led the US Endocrine Society to significantly revise its 2011 clinical practice guideline on vitamin D testing and supplementation, which had advocated screening for vitamin D deficiency (via the 25-hydroxyvitamin D [25(OH)D] blood test) in a large swath of the population, and supplementing quite intensively with either vitamin D2 (ergocalciferol) or D3 (cholecalciferol) "to achieve a blood level of 25(OH)D above 30 ng/ml" (that's 75 nmol/L).
The Endocrine Society's 2024 updated guideline recommends against population-wide screening for vitamin D deficiency, and openly acknowledges that there is insufficient evidence to determine the optimal blood level of 25-hydroxyvitamin D for disease prevention; that this level may vary by race/ethnicity or other sources of genetic variability; and hence that the dosage of supplemental vitamin D2 or D3 required to obtain an optimal blood level of 25-hydroxyvitamin D is not known.
There are many possible explanations for the disappointing results of vitamin D supplementation trials. For example, in the largest of these trials, the VITamin D and OmegA-3 TriaL (VITAL), baseline 25-hydroxyvitamin D levels were 77 nmol/L (31 ng/mL) in both the control and intervention group; relatively few participants had very low baseline 25-hydroxyvitamin D levels (below 30 nmol/L [12 ng/mL]); and participants allocated to the control group were permitted to continue taking up to 800 IU of vitamin D supplements per day (although only 5.6 per cent were doing so by the second year of the study, and 10.8 per cent by the fifth). Hence, critics have argued that all that VITAL proves is that people whose serum 25-hydroxyvitamin D level is already adequate don't get much benefit from taking 2000 IU of vitamin D per day (although there was a trend toward lower cancer mortality, and people with a healthy body mass index [below 25kg/m2, i.e. not overweight] did have reduced risk of developing invasive cancer).
But there's another potential explanation for the failure of vitamin D supplementation trials to deliver the results that observational studies predicted: reverse causation. That is, low serum levels of 25-hydroxyvitamin D may be the result of certain disease processes, rather than their cause. Let's explore the evidence for the reverse causation hypothesis.
The inflammation connection
Back in 2014, a systematic review of 290 prospective cohort studies and 172 randomised trials of major health outcomes and of physiological parameters related to disease risk or inflammatory status, concluded that
"The discrepancy between observational and intervention studies suggests that low 25(OH)D is a marker of ill health. Inflammatory processes involved in disease occurrence and clinical course would reduce 25(OH)D, which would explain why low vitamin D status is reported in a wide range of disorders."
Evidence that 25-hydroxyvitamin D1 is an acute phase reactant has been accumulating for several decades. The acute phase response refers to the large number of behavioural, physiologic, biochemical, and nutritional changes that occur during inflammatory states. Acute phase reactants are markers of inflammation, whose serum concentration either increases (positive acute phase reactants) or decreases (negative acute phase reactants) during both acute and chronic inflammatory states. Your doctor might, at some point, have run a blood test for C-reactive protein (CRP) to 'check your inflammation level'. CRP is a positive acute phase reactant, and is considered a highly sensitive marker of inflammation. Or your doctor might have expressed concern that you had 'low protein' when a serum biochemistry test found that you had low albumin; albumin is a negative acute phase reactant, and hence it is more likely that your low albumin was due to inflammation than to a dietary protein deficiency.
25-hydroxyvitamin D is, like albumin, a negative acute phase reactant. That is, its concentration drops during bouts of inflammation, whether acute (e.g. in response to infection or injury) or chronic (e.g. as an integral part of the pathology of atherosclerotic cardiovascular disease, cancer, and diabetes). The evidence that serum 25-hydroxyvitamin D levels fall as a consequence of the inflammatory state, rather than low levels of 25-hydroxyvitamin D being a cause of inflammation, is quite substantial:
There is an inverse correlation between serum CRP and 25-hydroxyvitamin D levels: the higher the CRP, the lower the 25-hydroxyvitamin D.
Obesity is characterised by a chronic inflammatory response, with multiple markers of inflammation consistently found to be elevated in obese individuals. A study of extremely obese individuals found an inverse relationship between serum 25-hydroxyvitamin D and three well-established inflammatory markers: highly sensitive CRP, interleukin 6 (IL-6) and tumour necrosis factor alpha (TNF-α).
Furthermore, the persistence of low 25-hydroxyvitamin D levels in obese patients despite aggressive supplementation regimes is exactly what one would expect if 25-hydroxyvitamin D was an acute phase reactant.
In patients undergoing elective knee or hip replacement surgery, none of whom were taking vitamin D supplements, serum 25-hydroxyvitamin D levels dropped from an average of 56 nmol/L (22 ng/mL) in the month before surgery, to 46 nmol/L (18 ng/mL), 48 hours after surgery. Serum vitamin D binding protein2 also fell from 334 to 298 mg/L. Meanwhile, average CRP increased from 5 mg/L before surgery to a walloping 116 mg/L afterwards. Patients who developed post-surgical infections were excluded from the study, demonstrating that the joint replacement surgery itself was a potent inflammatory insult.
The authors of this study concluded that
"Serum 25-(OH)D is a negative acute phase reactant, which has implications for acute and chronic diseases. First, serum 25-(OH)D is an unreliable biomarker of vitamin D status after an acute inflammatory insult. Second, it supports the notion that hypovitaminosis D may be the consequence rather than the widely purported cause of a myriad of chronic diseases."
Another study of patients undergoing elective knee replacement found that average 25-hydroxyvitamin D levels fell from 40 nmol/L (16 ng/mL) before surgery, to 26 nmol/L (10 ng/mL) within 6-12 hours post-surgery, dropping to a nadir of 23 nmol/L (9 ng/mL) at 24-48 hours post-surgery. At three-month follow-up, patients' serum 25-hydroxyvitamin D levels were still 20 per cent lower than their pre-surgical values.
In patients admitted to hospital for acute pancreatitis, serum 25-hydroxyvitamin D levels fell along with albumin and haemoglobin between day 0 (admission) and day 2, while CRP levels rose.
While there is a very high prevalence of low 25-hydroxyvitamin D levels in critically ill hospitalised patients, "no data exist to show that vitamin D supplementation improves organ function and mortality in critically ill patients" - again, exactly as one would expect if 25-hydroxyvitamin D was an acute phase reactant.
When critically ill patients who were at high risk for death, and had a baseline 25-hydroxyvitamin D level of under 50 nmol/L (20 ng/mL), were administered high-dose vitamin D3 supplementation, their average 25-hydroxyvitamin D shot up to 117 nmol/L (46.9 ng/mL), but they were just as likely as the placebo group to die within 90 days, and there was no advantage in other, nonfatal outcomes including length of hospital stay, severity of hypoxaemia, acute respiratory distress syndrome, acute kidney injury, and cardiovascular failure.
A systematic review concluded that there is consistent evidence that 25-hydroxyvitamin D levels drop after an inflammatory insult, with studies that measured 25-hydroxyvitamin D soon after the inflammatory insult finding an abrupt decline.
The implications of 25-hydroxyvitamin D being an acute phase reactant are profound. Roughly one third of US adults aged over 20 and UK adults aged 40–79 exhibit minor CRP elevation, as a consequence of low-grade inflammation caused by metabolic perturbation induced by conditions such as obesity, prediabetes and diabetes, and incipient cardiovascular disease. At least some proportion of the low 25-hydroxyvitamin D levels reported in observational trials, stem from its behaviour as an acute phase reactant rather than from genuine vitamin D deficiency. While it's possible to have truly inadequate production and/or intake of vitamin D and to be in an inflammatory state that reduces 25-hydroxyvitamin D levels, there is little doubt that 'vitamin D deficiency' is being overdiagnosed and overtreated because of the failure to recognise 25-hydroxyvitamin D as an acute phase reactant.
Let's consider why 25-hydroxyvitamin D is a negative acute phase reactant - that is, why its concentration drops as a consequence of inflammation. You'll (hopefully) recall from Part 2 that 25-hydroxyvitamin D is converted into the hormone calcitriol, by a number of different cell types including immune cells known as monocytes and macrophages. These cells are integral components of the innate immune system, our first line of defence against infection. When exposed to microbial antigens (that is, substances that are capable of stimulating an immune response), monocytes and macrophages ratchet up their production of calcitriol from circulating 25-hydroxyvitamin D, and switch on their own vitamin D receptor gene. The more calcitriol these cells make in response to infectious challenge, the greater will be the decline in the reservoir of 25-hydroxyvitamin D.
OK, that helps makes sense of rapidly declining 25-hydroxyvitamin D levels in people fighting infection, but what about the non-infectious conditions which lower 25-hydroxyvitamin D levels?
Systemic inflammation following surgery is known to be the result of the innate immune response, which activates calcitriol production in order to initiate tissue repair. Calcitriol levels have been found to shoot up after major cardiac surgery, remaining elevated for six weeks post-surgery.
One of the substances that stimulates monocytes and macrophages to produce calcitriol is lipopolysaccharide, which is a component of the cell wall of certain types of bacteria that form part of the human microbiome. Elevated plasma levels of lipopolysaccharide have been found in people with obesity and type 2 diabetes, and also predict the onset of diabetes. The lipopolysaccharide is believed to originate from translocation of bacteria, primarily from the gut, which is known to be dysbiotic - that is, to have an altered and disease-promoting microbial composition - in both obesity and diabetes.
Elevated plasma lipopolysaccharide is also found in both acute and chronic pancreatitis, and is responsible for severe sepsis, which is one of the major causes of death in critically ill patients.
In short, there are well-established mechanisms via which upregulation of calcitriol production could explain either chronically low 25-hydroxyvitamin D in the context of chronic inflammation, or a sudden drop in 25-hydroxyvitamin D in response to an acute inflammatory insult.
Supplemental futility
Administering vitamin D3 supplements in an attempt to drive up 25-hydroxyvitamin D, which is being converted to calcitriol at an accelerated rate as a direct consequence of inflammatory processes, is an exercise in futility. And just to ram the point home, administering calcitriol to critically ill patients with sepsis did not increase plasma levels of cathelicidin (a protein whose formation is stimulated by calcitriol), nor did it reduce inflammatory cytokines or improve clinical outcomes. When you're maxed out on calcitriol, adding more doesn't help.
In fact, it could even be counterproductive to supplement with vitamin D (or 25-hydroxyvitamin D, or calcitriol) while you're in a state of inflammation-induced low 25-hydroxyvitamin D with normal or elevated calcitriol, because you may exacerbate the condition that caused your low 25-hydroxyvitamin D level in the first place. How so?
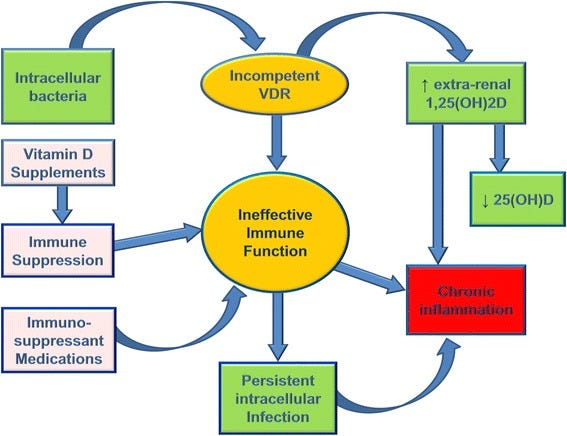
In order to protect themselves against the innate immune response, certain pathogens can inactivate the vitamin D receptor (VDR), with which calcitriol must bind in order to 'switch on' the hundreds (or possibly even thousands) of genes that respond to its messaging. This inactivation of the VDR sends the false message that calcitriol levels are too low, leading to upregulation of conversion of 25-hydroxyvitamin D into calcitriol. Because calcitriol is not able to bind to the inactivated VDR, it fails to initiate production of the enzyme that degrades it (part of the complex regulation mechanism described in Part 2). Meanwhile, the elevated calcitriol level decreases conversion of vitamin D2 and D3 into 25-hydroxyvitamin D. The upshot is that 25-hydroxyvitamin D levels drop while calcitriol may be normal or elevated - sometimes dangerously so. Supplementing with vitamin D in this scenario leads to immune suppression, allowing further proliferation of pathogens which only adds to the burden of chronic inflammation:
Cell wall deficient bacteria including Mycobacterium tuberculosis and Mycobacterium leprae are able to invade human cells and downregulate the VDR. So is Epstein-Barr virus, the agent associated with glandular fever (also known as infectious mononucleosis), and suspected to play a role in chronic fatigue syndrome and multiple sclerosis. So are Borrelia burgdorferi (the spirochete responsible for Lyme disease), Cytomegalovirus and Aspergillus fumigatus (a fungus which frequently colonises the lungs of those with compromised pulmonary function, including asthmatics and people with cystic fibrosis). And although, as previously mentioned, bacterial lipopolysaccharide triggers the synthesis of calcitriol, it also downregulates the VDR.
The intracellular pathogen-mediated derangement of VDR function may explain at least some cases of not just multiple sclerosis, but other autoimmune disorders as well, including Crohn's disease and rheumatoid arthritis.
You may remember from Part 3 that one of the few positive outcomes in VITAL was that 2000 IU of vitamin D daily for five years reduced new-onset autoimmune disease by 22 per cent. But according to some researchers, this may be merely kicking the can down the road:
"Vitamin D appears to have a positive effect on autoimmune disease due to immune system suppression [122, 134, 135] and immune suppression is considered therapeutically beneficial for autoimmune diseases [136, 137]. However, vitamin D proponents have failed to recognize that positive effects are due to the immunosuppressive effect of elevated 25(OH)D or to understand that immunosuppression is contraindicated because of the probable presence of intracellular infection. When the immune system is suppressed clinical disease markers and symptoms are reduced but immunosuppression does not address an underlying cause of persistent bacteria, thus relapse is common [138]."
Interestingly, curcumin (a constituent of the spice turmeric), gamma-tocotrienol and both omega-6 and omega-3 fatty acids are ligands for the VDR, which may be able to restore its competence when calcitriol is unable to activate the VDR due to microbial activity. All these compounds are characterised as anti-inflammatories and have been explored as treatments for people suffering from autoimmune conditions.
Monkeywrenching the system?
The vitamin D saga closely resembles the hormone replacement therapy fiasco, in which millions of menopausal women were prescribed steroid hormones - oestrogen with or without progestins - to treat a supposed 'deficiency' of these hormones, on the basis of observational studies. Subsequent randomised controlled trials failed to find the benefit which the observational studies had reported - namely, decreased risk of cardiovascular disease - and in fact reported an increased risk of stroke and pulmonary embolism. This led to a wholesale rejection of menopausal hormone therapy. More recently, subgroup analyses have identified certain categories of women who do appear to gain some benefit from menopausal hormone therapy - although I would argue that the focus on taking exogenous hormones distracts from advocacy for diet and lifestyle changes that would deliver more comprehensive health benefits, risk-free.
Likewise, a large swath of the population has been told that they are 'deficient' in vitamin D, and should take supplements in order to correct this deficiency, on the basis of observational studies. Randomised controlled trials have failed to validate the benefits inferred from observational studies, leading to influential authorities recommending against population-wide testing for, and supplementation with, vitamin D. It may well turn out that the pendulum swings too far in the opposite direction, and that certain subgroups who really would benefit from supplemental vitamin D, are deterred from taking it - although once again, my argument would be that they might benefit more from adopting diet and lifestyle changes that improved their vitamin D status.
Nonetheless, we should heed the lessons learned from the menopausal hormone therapy episode, and maintain a posture of epistemic humility - that is, admit that there is much that we still don't know. We are complex systems - unbelievably sophisticated bodies orchestrated by intricate, interlocking regulatory mechanisms - situated within other complex systems - the environments we inhabit. Attempting to monkeywrench this complex system by pouring a potent hormone into it, and assuming only good things will come from this intervention, is the height of hubris. We should know better by now.
In what I think might be the final instalment in this miniseries - at least for now - I will share some suggestions on optimising your vitamin D status using diet and lifestyle interventions. Stay tuned for that, in the next post.
And finally, this post has taken me approximately 20 hours to research and write. The breadth, depth and complexity of the vitamin D research literature is truly mind-bending. I make all my posts freely available to all readers, because I believe we all deserve access to information that helps us to take greater control over our health. But I rely on my small core of paid subscribers to provide this service to those who genuinely can’t afford it.
For information on my private practice, please visit Empower Total Health. I am a Certified Lifestyle Medicine Practitioner, with an ND, GDCouns, BHSc(Hons) and Fellowship of the Australasian Society of Lifestyle Medicine.
Just as a reminder, 25-hydroxyvitamin D (otherwise known as 24(OH)D, calcefidiol and calcediol) is the major circulating metabolite of the group of secosteroid hormones collectively known as 'vitamin D'. It is not biologically active, until acted upon by the 1α-hydroxylase enzyme, either in the kidneys or within certain other cells, to transform it into 1,25-dihydroxyvitamin D (otherwise known as calcitriol, or 1,25(OH)2D).
As explained in Part 3, most 25-hydroxyvitamin D circulates tightly bound to vitamin D binding protein (DBP). The blood test for 25-hydroxyvitamin D does not differentiate between bound and free or bioavailable 25-hydroxyvitamin D. Hence if the concentration of DBP falls, the level of 25-hydroxyvitamin D will drop too. In the study of joint replacement patients, there was increased urinary loss of DBP after surgery which accounted for some of the decline in 25-hydroxyvitamin D, with the remainder being accounted for by the redistribution of fluid from the blood vessels to the tissues, which is caused by other acute phase reactants.
Robyn, the research you've done for this four-part (so far) series is impressive and, as usual, the articles are well-written and easy to follow even for lay people like me. Thank you, as I'm among those who have been interested in knowing more about the usefulness of vitamin D supplementation. I look forward to your next installment where I understand you'll be addressing diet and lifestyle approaches for maintaining adequate vitamin D levels.
Meantime, I have a couple of questions. First, and while I recognize your vitamin D series is not promoting vitamin D supplementation as a general means for improving health, I wonder what you think about the fact that commercially available vitamin D supplements are in fact identical to what is used as rat poison. Do you think that's simply a matter of the dose making the poison, or are commercially available vitamin D supplements toxic regardless of dose?
Second, your series makes a compelling case based on published medical literature, including a number of RCTs, that with certain exceptions vitamin D supplementation is not generally associated with improvements in health or reductions in mortality. I'm also familiar more generally with much of your other work over the past few years, including things you've written (and said) about critical thinking and conducting research. In that regard, it is becoming well known, especially among those who are awake to the fraud and corruption that infects governments and institutions around the world, that the pharmaceutical industry long ago compromised the public health establishment, which now is completely corrupt and does the bidding of the pharmaceutical industry without regard for the welfare of the general public that it is supposed to serve. The corruption extends to the biggest and supposedly best medical journals. Even former editors of some of the most highly-regarded journals began warning many years ago that the pharmaceutical industry had so corrupted the journals that they can not be relied upon as accurate sources of medical information. Clinical studies often are designed to fail, published results often are intentionally misleading, and it is not unheard of for study results and even the underlying data sets to be entirely falsified. We saw that in spades during the Covid-19 event, with corrupt insiders using designed-to-fail studies and falsified data sets to disparage safe and effective medications like hydroxychloroquine and ivermectin and to promote highly profitable and very dangerous alternatives like the experimental Covid-19 injections and toxic therapeutics like remedesivir. Similar but less well known fraud and corruption has been going on for decades and infected the clinical studies and medical journal reporting that ultimately led to the licensing and approval of other toxic drugs like SSRIs, statins, and more recently the new-fangled and extremely dangerous weight loss drugs.
In short, the pharmaceutical industry does not exist primarily to help people improve their health. To the contrary, it is profit-driven and derives benefit from chronic illness (and, arguably, keeping people sick). Given that it controls what the medical journals publish, I've concluded nothing they publish can be trusted. With that in mind, I wonder whether medical literature that discounts the utility of vitamin D supplementation is reliable -- after all, it would not seem to be in the best interests of the pharmaceutical industry if something like vitamin D supplementation actually helped improved people's health and made them less reliant on toxic pharmaceuticals.
Stated differently, if Robyn Chuter designed a study to determine whether vitamin D supplementation is safe and effective for improving immune system function and general health, I would have no doubt the study would be well designed, the reported data would be genuine, and the reported results would honestly and accurately reflect actual outcomes. I have no confidence in other researchers whose motivations and backgrounds are unknown to me, and the fact their work might get published in a medical journal I already know to be corrupt likely would cause me to disregard their study before reading the first sentence.
I totes agree with below writers comments. This is an excellent article..and as uusual Im so impressed by the indepth research you have done robyn. Changes my view on vit d.
I like the diet n lifestyle theory personally...I think thats why we have those receptors...but eagerly await your nxt publication. Well done.