


Sharpening Hanlon's Razor against granny-killers
Revisiting the incompetence vs malice argument in the light of Australia's ongoing geronticide.

Back in January 2022, I wrote an article titled Is Hanlon’s Razor sharp enough for COVID-19?, in which I asked whether we should be following the advice of Robert Hanlon - that is, to "never attribute to malice that which is adequately explained by stupidity" - when it came to the behaviour of politicians and bureaucrats during the manufactured COVID crisis.

Since then, I've had many conversations on this topic, and read and listened to commentators with a variety of points of view. The exchange between the German academic who writes under the pseudonym Eugyppius, and fellow trenchant critic of COVIDiacy, Igor Chudov, in these three posts is a superlative summary of the conspiracy-by-evil-people vs emergent-phenomena-of-declining-institutions-populated-by-deadheads debate.


It's also a model of respectful debate between people who disagree with each other on important points, and should be read for that reason alone - especially in the wake of the Twitterstorm that erupted when Dr Peter Hotez refused to accept Joe Rogan's invitation to debate Robert F. Kennedy Jnr on the latter's alleged 'vaccine misinformation', on his podcast (note that Rogan's initial tweet alone garnered 210,900 likes and 11,800 replies, most of them in favour of the debate that Hotez refused to participate in):
Hanlon's Razor returned to the top of my mind when a subscriber, and frequent correspondent, Mick, sent me a link to the latest version of a document titled 'COVID-19 outbreaks in Australian residential aged care facilities: National snapshot'.
This document, published by the Department of Health and Aged Care of the Federal government, is a "weekly report [which] provides a snapshot of data on the impact of COVID-19 in residential aged care facilities nationally."
In it, we learn that:
"As at 8:00 am 22 June 2023 there are 1,880 active COVID-19 cases in 292 active outbreaks1 in residential aged care facilities across Australia. There have been 99 new outbreaks, 42 new resident deaths and 1,592 combined new resident and staff cases reported since 15 June 2023."
COVID-19 outbreaks in Australian residential aged care facilities: National snapshot (23 June 2023)
Cast your mind back to 2020 and 2021, when every 'case' of COVID-19 was breathlessly reported in every news update of every television and radio station, and on the front page of every newspaper. Remember those daily press conferences when premiers and their health ministers sombrely intoned the numbers of (supposed) COVID-related hospitalisations and deaths that had occurred since their last appearance before the Mockingbird media? Yeah, so last week, 42 elderly institutionalised people bought the farm, (supposedly) of COVID-19, and no one in the media, or government, gave a crap.
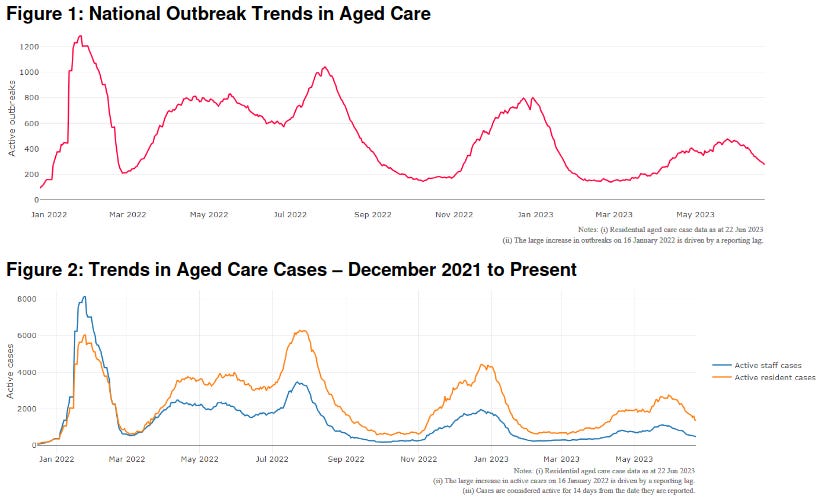
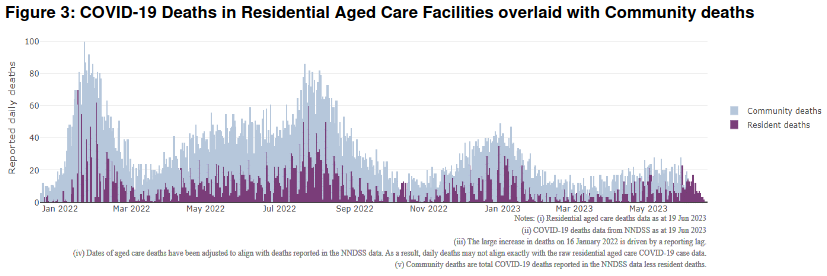
On top of that, figures from the article demonstrate that there have been multiple surges of outbreaks, cases and deaths attributed to COVID-19 in aged care facilities since January 2022 (which show an oddly coincidental correspondence with 'vaccination' drives, but we'll return to this point later), and once again, there has been deafening silence both from the corridors of power and the legacy media:
We also learn from the report that:
"71,304 prescriptions for Lagevrio (Molnupiravir) have been issued to residents in residential aged care facilities, with a further 5,501 prescriptions for Paxlovid (nirmatrelvir + ritonavir) also issued since 28 February 2022 and up to 18 June 2023."
COVID-19 outbreaks in Australian residential aged care facilities: National snapshot (23 June 2023)
Oh, would that be the molnupiravir that the National Clinical Evidence Task Force (NCET) advised, back in December 2022, should not be routinely used for COVID because it "does not have an impact on the combined endpoint of hospitalisation and/or mortality in multiply-vaccinated adults with mild COVID-19 and one or more risk factors for disease progression"?

Would that be the molnupiravir that isn't even included on NCET's decision tool, 'Drug Treatments For At Risk Adults With COVID-19 Who Do Not Require Oxygen', which would presumably cover all people who are being treated for COVID-19 within an aged care facility?
I guess they have to do something with the massive stockpile of this next-to-useless drug that promotes transmissible viral mutations, is possibly carcinogenic (cancer-causing), and resulted in more deaths from COVID-19 than placebo in some randomised clinical trials, that they ordered back in early 2022.

Why not palm it off on helpless residents of old folks' homes? After all, if you give it to everyone who tests positive to SARS-CoV-2, you can easily disguise any excess deaths that it's causing, because there's no control group to compare outcomes.

We also learn from the report that:
"People living in residential aged care homes remain a high priority for the Government’s COVID-19 vaccination program. The Department is continuing to communicate with both the aged care and primary care sectors, reinforcing the importance of uptake and promoting the 2023 booster dose via regular newsletters, bulletins, social media videos and webinars.
All aged care residents who have not had a COVID-19 vaccination, or a COVID-19 infection within the last 6 months, continue to be offered a 2023 booster dose. The added protection from vaccination is especially important for aged care residents and will help reduce the risk of severe illness or hospitalisation."COVID-19 outbreaks in Australian residential aged care facilities: National snapshot (23 June 2023)
By "added protection", do they mean the increased risk of infection with every dose of 'vaccine' that was demonstrated in the study of 51 017 employees of the Cleveland Clinic, published in April 2023?
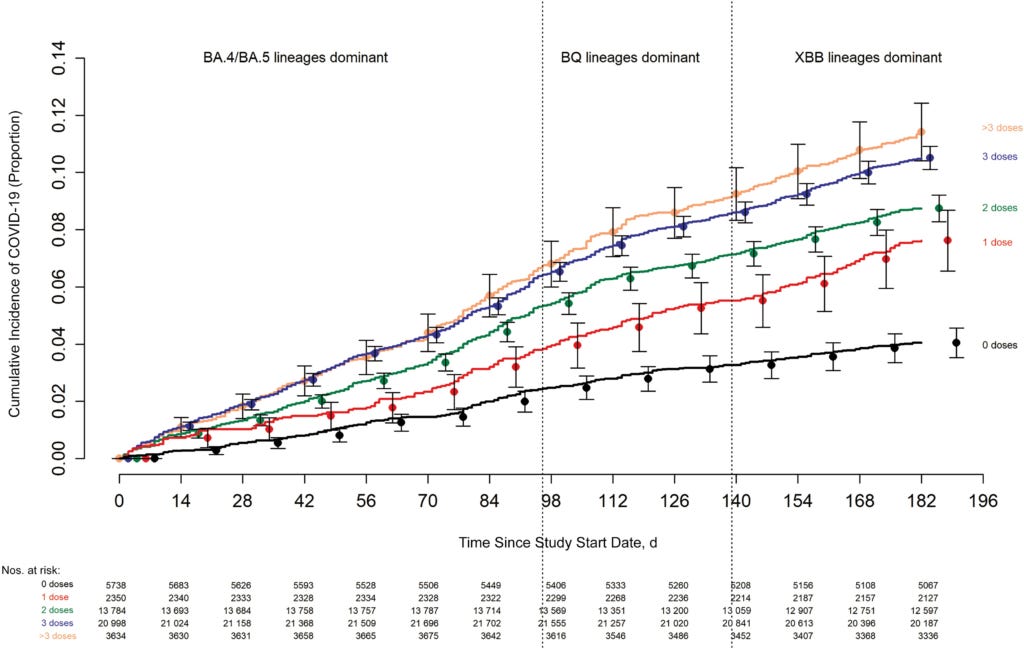
Here's another view of the data from this study, which shows, in the authors' own words, "the greater the number of vaccine doses previously received the higher the risk of COVID-19":
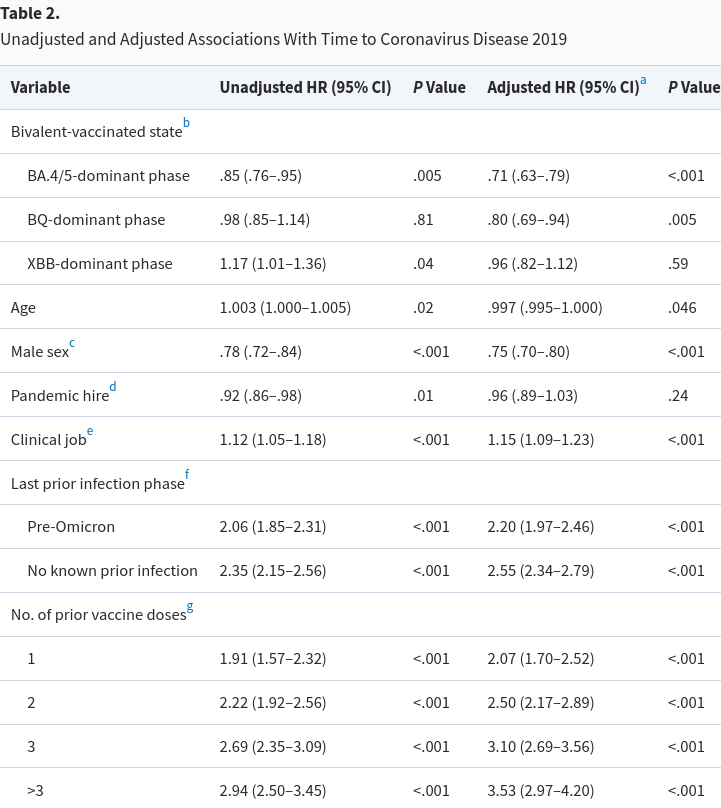
The Cleveland Clinic study authors explicitly stated that "A protective effect of bivalent vaccination could not be demonstrated while the XBB strains were dominant". Those strains are still dominant in Australia, accounting for 72 per cent of all sequences uploaded to AusTrakka in May-June 2023.
But never fear, the smart people running the Commonwealth health department were super-proud to report that, in the week since the previous update, 4282 aged care facility residents had been jabbed with "a 2023 booster dose". According to advice issued by the Australian Technical Advisory Group on Immunisation (ATAGI) in February 2023, the preferred product for a "2023 booster dose" in the nursing home-age group is - you guessed it - the completely useless (and in fact, risk-increasing) bivalent shot.
Ah, but but but, I hear the Branch Covidians protest, that Cleveland Clinic study was conducted in healthy, working-age adults, so the results can't be extrapolated to elderly residents of aged care facilities. And we know the COVID jabs reduce the risk of hospitalisation and death in this population because there's lots of Vaccine Science™ that says so.
That's where this paper, written by Dr Wilson Sy comes in. Dr Sy was formerly head of research for the Australian Prudential Regulatory Authority (APRA), and executive at the Australian Securities and Investment Commission (ASIC) and the Australian Treasury. In 2018, Sy became a whistleblower on the regulatory capture of APRA, ASIC and Treasury by the banking industry, accusing these agencies of creating "fake regulation" which benefits financial predators (including the major banks) at the expense of the public.
Sy turned his impressive analytic skills to Australia's COVID response, producing a series of papers on the failure of the so-called vaccines to 'end the pandemic' and the evidence that they were actually driving excess mortality. The third paper, 'Simpson's Paradox in the correlations between excess mortality and COVID-19 injections: a case study of iatrogenic pandemic for elderly Australians' explains why the studies purporting to show that the shots decrease the risk of serious illness, hospitalisation and death are just plain wrong.
In a nutshell, deaths that occurred within two weeks of the first shot were arbitrarily categorised as "unvaccinated" deaths, whilst in those who survived the initial injection, there was a peak of excess mortality roughly five months later (a temporal separation confirmed in datasets from several other countries, which intimates that the injections are exacerbating terminal conditions such as heart disease, cancer and neurodegenerative disease):
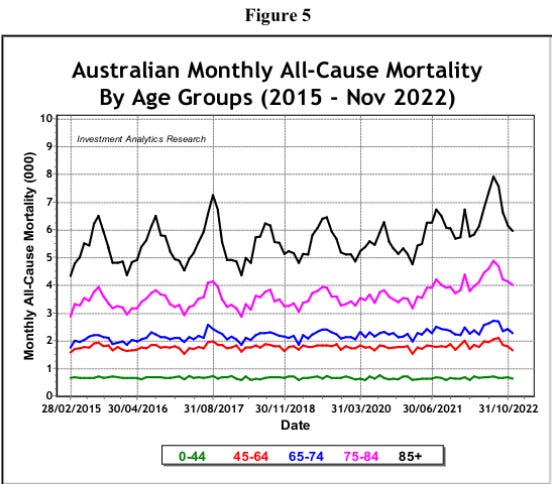
As Sy graphically illustrates, that excess mortality has been particularly concentrated in the 75+ age group - in other words, the group most likely to be in residential aged care - and it only began after the roll-out of the experimental injections in 2021:
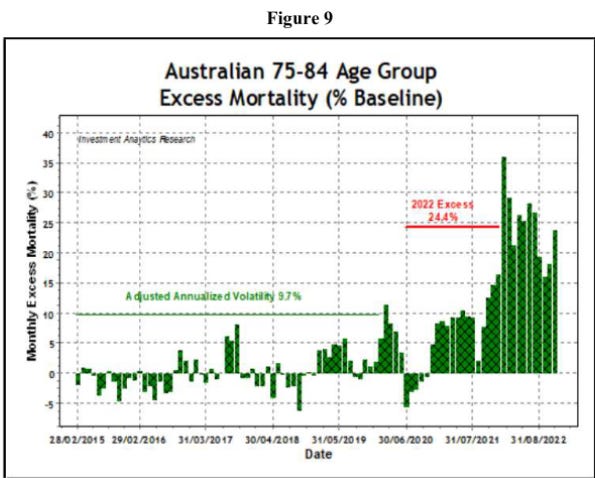
Sy further breaks out monthly excess mortality figures in the 75-84 age group to illustrate just how historically anomalous the current levels of excess deaths are - as high as seven times the 2015-2019 baseline:
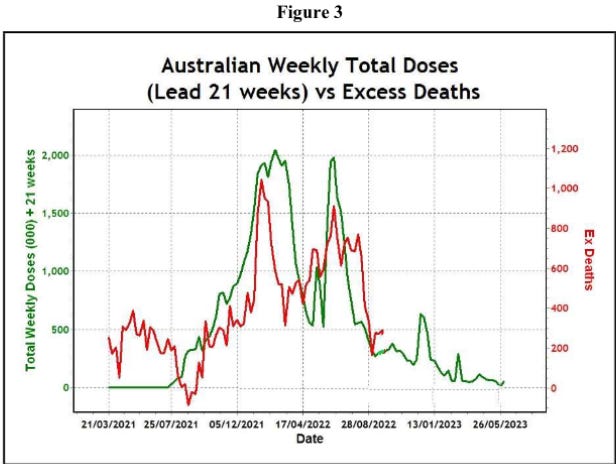
Graphing the monthly total doses of experimental injection against excess deaths in the 75+ age group, lagged by 5 months, makes the correlation very obvious:

Sy's concluding remarks don't pull any punches, and demonstrate which side of the Hanlon's Razor argument he inclines towards:
"Earlier epidemiological evidence that COVID injections reduce illness and death has been refuted as an example of Simpson’s Paradox; instead, the evidence has shown increased iatrogenic [treatment-caused] deaths. Without taking the precaution of investigating the abnormally high excess deaths, Australia has continued to prioritize the elderly for COVID injections which the elderly cannot usually refuse if they are in residential aged-care facilities.
The longer the authorities delay stopping widespread injections to conduct a thorough investigation into the causes of excess deaths in Australia, the stronger is the implication that the excess deaths in the elderly are deliberate policy, which is in effect iatrogenic geronticide. Geronticide is a serious violation of human rights, because it is a morally reprehensible criminal act to target intentionally older adults based on their age."
As Sy points out, monthly excess mortality has continued to run at unprecedentedly high levels since the data analysed in his paper, and yet in March 2023, Australian senators, by a slim majority, voted against launching an inquiry into these unexpected deaths.
When the Commonwealth health department is hell-bent on continuing to inject defenceless elderly people with an endless series of boosters that have been shown to increase the risk of infection, and the Senate refuses to examine the reasons for the excess deaths occurring in the entire population (and particularly concentrated in the nursing home-aged demographic), it is hard to defend the position that stupidity, rather than malice, explains this bizarre behaviour.
What do you think? Is this country run by incompetent clowns, or cold-blooded murderers?
For information on my private practice, please visit Empower Total Health. I am a Certified Lifestyle Medicine Practitioner, with an ND, GDCouns, BHSc(Hons) and Fellowship of the Australasian Society of Lifestyle Medicine.
In the document, "An outbreak is defined as at least 1 positive case in a resident or 2+ cases in staff."
I feel it is becoming increasingly difficult to attribute what is happening solely to stupidity. At some higher level it appears manufactured and intentional, any level below that can be explained by various factors, wilful blindness, we turn a blind eye in order to feel safe, to avoid conflict, to reduce anxiety and to protect prestige. From Margaret Heffernan, "by challenging our biases, encouraging debate, discouraging conformity, and not backing away from difficult or complicated problems – we can be more mindful of what's going on around us and be proactive instead of reactive."
Denis Rancourt has also done some great work along the lines of Dr Wilson Sy
https://denisrancourt.ca/entries.php?id=125&name=2022_12_20_probable_causal_association_between_australiarsquos_new_regime_of_high_all_cause_mortality_and_its_covid_19_vaccine_rollout
https://denisrancourt.ca/entries.php?id=126&name=2023_02_09_age_stratified_covid_19_vaccine_dose_fatality_rate_for_israel_and_australia
I always appreciate the depth and scope of your articles/arguments.
I see a lot of people, myself included, overcoming the assumption that humans are basically good, our systems are basically working, psychopaths are rare, we would never conduct genocide in the modern age, science, stats, data is even remotely trustworthy etc. etc. This is a good thing. Definitely malevolence.....
However, it's important to note how easy it is to obfuscate this issue, or to note how it may seem simple, but actually be more complex. Consider a single study providing evidence of dramatically variable batches: https://childrenshealthdefense.org/defender/pfizer-biontech-covid-vaccine-placebo/
Was/is this:
- 'good actors minimising the genocide from within the apparatus'? - yay humanity
- evidence of incompetence in manufacturing being the major cause of the deaths? ( I suggest no, see people like Mike Yeadon dismissing that possibility very convincingly (https://expose-news.com/2022/01/10/mike-yeadon-covid-injections-are-toxic/))
- Part of the plan of general general war on reality and understanding?
- Partly failed malevolence? (they would have preferred to kill more, but human error actually led to less deaths)
- Part of some harder to decipher plan from those who conspired?
- Evidence of even more targetted killings? (eg. the deadlier batches went to certain demographics for a reason)
- Yet another study biased by money or corrupted data?
- A foreward thinking escape clause from Crimes Against Humanity trials?