


Cholesterol and depression: What’s bad for the heart is bad for the brain
Major depressive disorder is linked to higher total and LDL cholesterol levels... and that means diet and lifestyle changes can help your mood as much as your body.

N.B. I hate those stupid trigger warnings that encourage grown adults to believe that they'll be permanently psychologically harmed by reading about upsetting topics. But yeah, this post discusses suicide - a lot - so if you find that triggering, consider yourself warned. Anyhow...
In the last post, I laid out the evidence from multiple types of studies, that elevated LDL-cholesterol and/or apolipoprotein B levels increase the risk of cardiovascular disease, and that plant-rich diets decrease LDL-C and apoB. But one of the criticisms of a plant-based diet that I've read on pro-meat blogs is that excluding animal products may increase a person's risk of psychological and mental disorders, including dementia and depression, by decreasing their cholesterol levels.
I’ve even seen the argument put by vegans, that people on 100% plant-based diets should eat coconut oil in order to prevent their serum cholesterol level from becoming ‘too low’.
There's a familiar pattern to all such furphies: a physiological or biochemical fact is misinterpreted, either deliberately or through sheer ignorance, to spin a completely fictitious story.
In this case, the physiological fact is that our brains contain cholesterol. A lot of cholesterol. The human brain contains approximately 20 to 25 per cent of the body's total cholesterol, despite making up only about 2 per cent of body weight. Cholesterol is a structural component of the myelin sheaths that wrap around the axons of each neuron (‘brain cell’), forming the white matter of the brain. Myelin acts as an electrical insulator and conductor, speeding up the transmission of messages from one neuron to the next. The cell membranes of neurons (the working units of the brain) and astrocytes (cells that support the neurons) also contain cholesterol, which helps them to maintain their shape and transmit electrochemical signals to one another.
However, as I mentioned in Is low cholesterol bad for you?, the protective filter known as the blood-brain barrier normally prevents any cholesterol that’s travelling through the bloodstream from getting into the brain. Hence, brain cells must make their own cholesterol – which they’re perfectly capable of doing, using the enzyme HMG-CoA reductase to transform components of carbohydrate and fats into acetyl-CoA, and then, via a multistep process, into cholesterol. There is also substantial recycling of 'used' cholesterol in the brain; whereas the half-life of plasma cholesterol is only a few days, the half-life of cholesterol in the adult brain is between six months and five years.
Hence, even the strictest vegan’s brain is amply supplied with cholesterol, regardless of how low his or her serum cholesterol may be, and whether he or she eats coconut oil. In a nutshell (or a peapod, perhaps?), low serum cholesterol does not cause low brain cholesterol.
Cholesterol and Alzheimer's disease
Furthermore, the function of neurons is impaired just as much by an excess of cholesterol as by a deficiency of it. For example, the brain cell membranes of people with Alzheimer's disease have been found to be overloaded with cholesterol, and the accumulation of cholesterol in cell membranes accelerates as the condition progresses.
In addition, there is a substantially increased risk of Alzheimer's disease in people who carry the APOE4 gene variant. The APOE gene codes for production of apolipoprotein E, which is - as you'll hopefully remember from What is high cholesterol, what is low, and why should you care? - a protein that helps transport lipids (fats and cholesterol) in the blood. About 25 per cent of the population carries one copy of the APOE4 allele, while 2 to 3 per cent carry two copies - essentially meaning that all the apolipoprotein E that they produce is of the apolipoprotein E4 (ApoE4) conformation. ApoE4 increases cholesterol production both throughout the body and in the brain, as well as impairing cholesterol efflux from neurons and allowing cholesterol from the peripheral circulation to enter the brain by damaging the blood-brain barrier. The result is abnormally high levels of cholesterol within the brain and specifically, within neurons.
Low cholesterol, depression and suicidal behaviour
Another frequently-used gambit of the high-cholesterol-is-good-for-you crew, is to cite studies linking a low cholesterol level with a higher risk of suicidal ideation (i.e. thoughts of committing suicide), suicide attempts, and violent behaviour, like this one, this one, this one and this one, to argue that reducing serum cholesterol is bad for mental health.
However, the connection between suicidality and cholesterol is, to put it mildly, complicated. Multiple studies and meta-analyses have found no link between low serum lipid levels and suicidality, including this one, this one, this one and this one while others have found a positive association (i.e. higher risk of suicidal behaviour in people with higher serum cholesterol), including this one, this one, this one, this one and this one.
Practically all of the studies that have reported a negative association between serum cholesterol and suicidality (i.e. lower serum cholesterol found in people who exhibited suicidal behaviour) have been cross-sectional, meaning that participants' cholesterol level was measured at the point at which they were hospitalised after a suicide attempt, or after expressing suicidal ideation. In contrast, many of the studies that have reported the opposite finding - more suicidal behaviour in people with higher cholesterol levels - have been prospective, meaning that participants' cholesterol levels were measured at baseline, and those who subsequently exhibited suicidal behaviour were found to have had higher serum cholesterol at baseline.
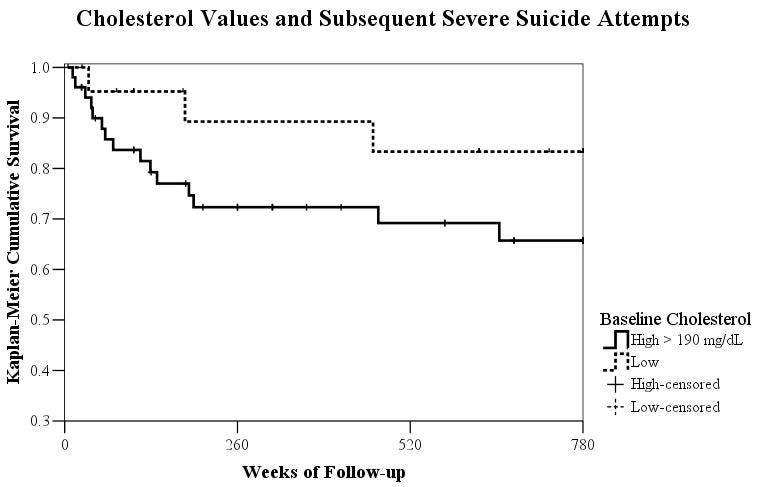
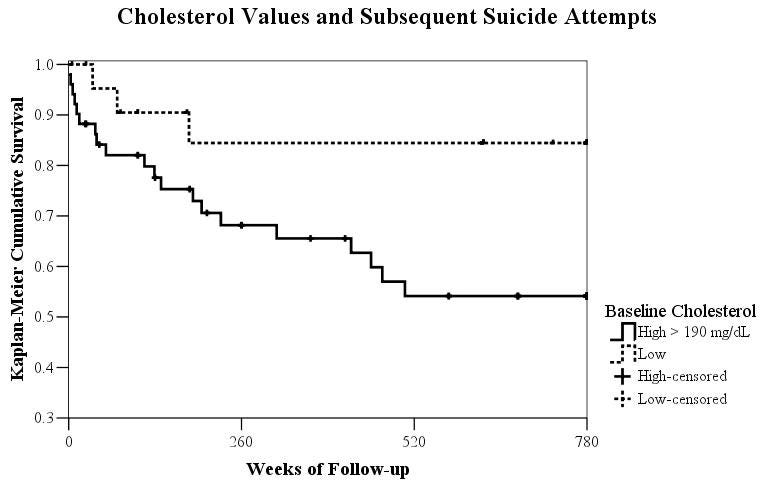
One hypothesis that might explain this peculiar pattern, is that high serum cholesterol predisposes to eventual suicidal behaviour, but that intensification of suicidal ideation, and suicide attempts themselves, are accompanied by an acute decline in serum cholesterol. A study which both measured the cholesterol level of suicide attempters at hospital admission, and then followed them up over time, provides evidence for this hypothesis. The average cholesterol level of people who were admitted to a psychiatric hospital just after a serious suicide attempt, was significantly lower than that of depressed patients who had not attempted suicide. But patients with high serum cholesterol (above 190 mg/dl, or 4.9 mmol/L), were much more likely to attempt suicide over the next fifteen years:
An analagous situation is observed with acute myocardial infarction: high serum cholesterol predisposes to having a heart attack, but total and LDL cholesterol drop precipitously in the aftermath of heart attacks. (I discussed this phenomenon, and its misinterpretation by saturated fat enthusiasts, in Diving down the low-carb rabbit hole – Part 1.)
A major piece of evidence supporting the hypothesis that elevated serum cholesterol predicts future suicide risk, is that depressed people are more likely to experience suicidal behaviour, and higher serum total cholesterol, LDL cholesterol and triglycerides are found in people suffering from depression and bipolar disorder, especially bipolar depression.
For example, a study published in June 2019 by German researchers compared blood lipid levels in people who were suffering from a major depressive episode, people whose major depressive disorder had remitted, and healthy controls who were free of depression. Not only did the German team find that LDL cholesterol levels were higher in people who were currently suffering from major depression, but those with the most severe depressive symptoms (as measured by the Hamilton Depression Rating Scale) had the highest total and LDL cholesterol and triglycerides.
Polish researchers reported similar findings in 2015: people suffering from both unipolar and bipolar depression had elevated total and LDL cholesterol, and in addition, elevated fasting plasma glucose.
Here's another piece of evidence for the high-cholesterol-predisposes-to-future-suicide hypothesis: Remember the APOE4 allele, which leads to both high serum cholesterol and greater accumulation of cholesterol within the brain? A 2018 study of Mexicans who carry the APOE4 allele found that they were almost five times more likely to commit suicide. (They were also more than 23 times as likely to have an advanced stage of a key Alzheimer's-related pathology, neurofibrillary tangles, as same-aged people who had non APOE4 alleles.)
Also in 2018, a Brazilian research team found that young adults suffering from depression with anhedonia – an inability to experience pleasure from activities that they had previously enjoyed – had a higher prevalence of metabolic syndrome (elevated glucose, triglycerides, total cholesterol and LDL cholesterol, accompanied by decreased HDL cholesterol level, abdominal obesity and high blood pressure) compared to those who were depressed but not suffering from anhedonia. Anhedonia is considered to be a cardinal symptom of major depressive disorder.
Cause or effect?
Alert readers may be asking the ‘chicken and egg’ question at this point: does deranged lipid and glucose metabolism cause depression, or does depression cause deranged lipid and glucose metabolism? Most researchers believe that it’s both.
On the one hand, once people become depressed (and especially if they develop anhedonia) they’re less likely to exercise, and more likely to make unhealthy food choices. The reward circuitry in the brains of people with anhedonia shows reduced activation in response to normal stimuli, which may drive them to overeat hyperpalatable food in a desperate attempt to wring some skerrick of reward signalling out of their unresponsive brains. Overeating and underexercising tend to lead to weight gain, dyslipidaemia and reduced insulin sensitivity.
On the other hand, major depressive disorder is characterised by immune-inflammatory alterations that also occur in cardiovascular disease, insulin resistance and type 2 diabetes. The chronic inflammatory state generated by eating a Western diet-style and being sedentary may increase the risk of depression, just as it increases the risk of cardiometabolic disease.
In other words, what we think of as ‘mental health issues’ may perhaps be more accurately described as psychological manifestations of the metabolic dysfunction that arises when we don’t live in a manner congruent with our species' physiological and psychological adaptations.
When exposed to a Western-style diet high in saturated fat, refined carbohydrates and animal protein, and low in fibre, complex carbohydrates and phytonutrients, coupled with social poisons such as smoking, and a sedentary lifestyle, our blood vessels become atherosclerotic; our muscles and livers clog up with fat, destroying our insulin sensitivity; and our brains become depressed:
"Several reports in the literature have suggested that vascular risk factors—such as smoking, hypertension, and increased serum cholesterol—play a putative role in the etiology of depression. There is also neuropathological evidence for an excess of atheromatous disease in the aortic and cerebral vessels in late life depression (Thomas et al., 2001). On the basis of such findings, several researchers have postulated a ‘vascular depression’ hypothesis (Alexopoulos et al., 1997; Krishnan et al., 1997). This hypothesis argues that for a subset of patients, depression may be caused by cerebrovascular disease manifesting as small lacunes in the subcortical gray and the white matter. These lesions would then disrupt the prefrontal systems related to mood regulation or the white matter pathways connecting these areas with other parts of the brain (Alexopoulos et al., 1997)."
Cholesterol in mood and anxiety disorders: review of the literature and new hypotheses
In addition, loneliness and social isolation are linked to increased levels of systemic (body-wide) inflammation which exacerbates both metabolic dysfunction and depression.
Of course, the balance of precipitating factors will vary for each depressed individual, and they become mutually reinforcing: once depression has set in from any cause, low motivation, fatigue and anhedonia conspire to make it harder to make healthy lifestyle choices, and the resulting poor nutrition, lack of exercise and social withdrawal worsen the depression.
As to what might precipitate a drop in serum cholesterol around the time that people exhibit suicidal behaviour, there are a couple of promising leads. Severely depressed people commonly lose weight as they lose interest in food; malnutrition and weight loss both lower total cholesterol, LDL-C and HDL-C.
Then there's interleukin-2 (IL-2), a cytokine produced by T cells as part of the inflammatory response, which has been shown to cause a decrease in serum cholesterol. Does thinking about killing yourself induce an inflammatory response? That would make complete sense, since inflammation is a defensive response to acute stress, and your own impending death is about as great a stress as one could imagine.
I also wonder if the phenomenon has some relationship with the terminal decline in cholesterol - the fall in cholesterol levels observed as people approach the end of life - that I discussed in Is low cholesterol bad for you? Is it possible that the body begins to prepare for death when the mind has decided to induce it? I don't know, but what I do know is that the mind is so powerful in its influence over biological functions, that in people with dissociative identity disorder (formerly called multiple personality disorder), each alter (distinct personality) can have different visual function, handedness, allergic sensitivity and regional blood flow patterns in the brain. So it doesn't seem too much of a stretch to imagine the suicidal mind initiating a body-wide shut-down process that leads to reduced serum cholesterol.
Take-home messages
The poet Sylvia Plath graphically described the depression which ultimately claimed her life as “an owl’s talons clenching my heart”. While we wait for researchers to tease out all the intricate pathways which link diet and lifestyle choices to health outcomes, we can all take simple but powerful actions to either reduce our risk of becoming depressed, or to help ourselves (or those we care about) to loosen those owl’s talons.
Eat a diet rich in whole or minimally-processed plant foods, high in fibre and low in the types of fats associated with metabolic dysregulation – particularly saturated and trans fats.
Move your body every single day: build physical activity into your routine; the more vigorous, the better.
Spend time outdoors in nature, as often as possible but at least once per week.
Prioritise sleep: aim to sleep to satiety (i.e. sleep long enough that you wake spontaneously, feeling refreshed) every night; and maintain a sleep schedule that’s in sync with your body’s circadian rhythm – aim to be in bed by no later than 10 pm each night, and wake within an hour of sunrise. (Read my article Sleep yourself slim and healthy to learn more about the effects of sleep deprivation on metabolic function.)
Engage in activities that you find personally meaningful, and which allow you to make a contribution to the well-being of others.
Invest your energies into building strong relationships with actual human beings rather than getting lost in the online world.
And finally, this post has taken me approximately 20 hours to research and write. Sifting through endless studies and extracting the nuggets of actionable information is an arduous business! I make all my posts freely available to all readers, because I believe we all deserve access to information that helps us to take greater control over our health. But I rely on my small core of paid subscribers to provide this service to those who genuinely can’t afford it.