
The dark side of weight loss: Are GLP-1 agonists putting patients at risk for blindness, depression and suicidal thinking?
Are vision loss and suicidality an acceptable trade for weight loss? Drugmakers, regulators and doctors seem to think so.

Do you ever get the feeling that you're living in Groundhog Day? I sure as heck do.
The same criminally insane people who started illegal wars and called for regime change everywhere else in the Middle East (remember how that turned out?) have launched another illegal war and are now pushing for regime change in Iran.
The same scammers who hatched the utterly bogus 2009 H1N1 'swine flu' scare in order to activate sleeper contracts with their Big Pharma buddies, leading to a multibillion dollar payday for GlaxoSmithKline, which produced a vaccine (Pandemrix) that caused astonishingly high rates of serious disorders including narcolepsy, facial palsy, convulsions and death and yet was kept on the market long after the pharmacovigilance systems of multiple governments had detected clear safety signals... well, they did it all again with 'COVID-19', and since the pandemic disaster capitalism machine continues to grind on inexorably, you can bet your booty that another highly-profitable (but not for you) scamdemic will be launched at some point in the not-too-distant-future.
And the same rotten-to-the-core industry that brought you the previous 25 anti-obesity medications withdrawn for safety reasons between 1964 and 2009 (and the bonus one taken off the market in 2020) is now promising that their new miracle weight loss drugs - the GLP-1 agonists such as Ozempic, Wegovy and Saxenda - will solve the obesity crisis for real this time, while being as safe as mother's milk. Cue Sonny and Cher.
In case you missed any of the previous miracle weight loss drugs that helped people fit into smaller coffins, here they are:
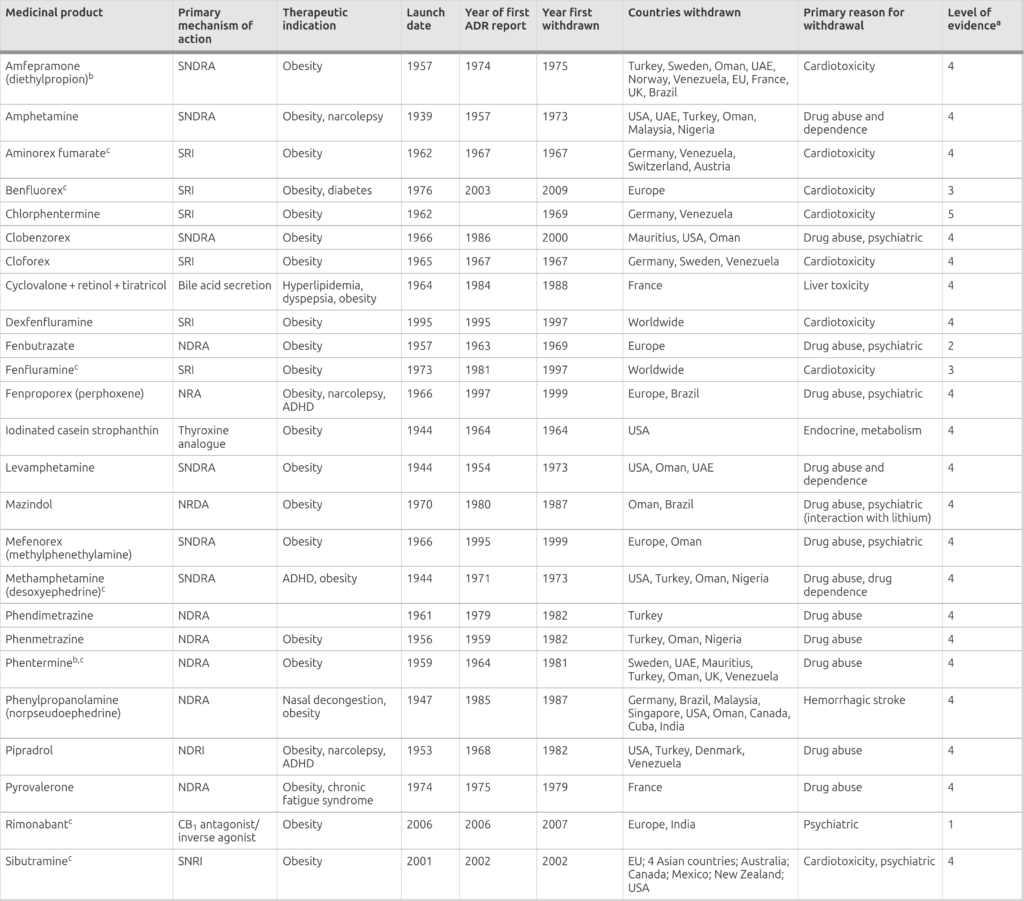
Oh yeah - and the one withdrawn in 2020, Belviq, was pulled for causing cancer. What an amazing business model - fleece 'em for the weight loss, and fleece 'em again for the cancer treatment. As an added bonus, Belviq also caused serotonin syndrome, and valvular heart disease and mood changes including depression and suicidal thoughts (more on that last point, shortly).
Luckily, the good folks in the drug and biotech industry are not deterred by their record of abject, catastrophic failure, and are determined to keep pushing on to ever greater glory.
And that brings me to two recently-published papers on emerging adverse effects of GLP-1 agonists - the first one reporting a more than two-fold higher risk of neovascular age-related macular degeneration, and the second outlining the mechanisms via which these drugs could induce suicidal ideation in genetically susceptible individuals.
Blinded by their plight
Previously, I discussed the association between the use of the GLP-1 agonist semaglutide (marketed as Ozempic and Wegovy) and nonarteritic anterior ischemic optic neuropathy (NAION), an untreatable eye condition that can cause blindness. NAION is nasty, but fortunately quite rare, with an incidence rate between two and ten cases per 100 000. So although the 4.3-7.7 times higher likelihood of developing NAION in GLP-1 agonist users than non-users is disturbing, the absolute magnitude of the risk is still low.
Age-related macular degeneration (AMD), on the other hand, is the leading cause of irreversible legal blindness in Australia, and the neovascular subtype accounts for the vast majority of AMD-related vision loss leading to blindness even though it is far less common than the 'dry' form of the condition. Neovascular AMD - also called 'wet' or 'exudative' AMD - is characterised by the formation of abnormal blood vessels under the central part of the retina, which is called the macula. The macula is responsible for high-resolution, colour vision.
These fragile blood vessels leak blood, fluid and cellular lipids (fats) into the retina, causing damage that may initially present as blurry or distorted vision, straight lines appearing curved or wavy, or new blind spots, but it can lead to rapid and irreversible vision loss. Three in every 10 000 US adults aged 60-64 have neovascular AMD, rising to 28 per 1000 in 75-79 year olds and 198 per 1000 in people aged over 90. Women have a higher risk than men.
So the recent publication of a population-based, retrospective cohort study that found that diabetics who used GLP-1 agonists more than doubled their risk of this already common and highly disabling condition, compared to diabetics who used other treatments, is extremely alarming.
Drawing on a Canadian medical database containing records from over a million patients, the researchers identified 46 334 individuals with diabetes who had taken a GLP-1 agonist for at least six months. Each of these was matched with two other diabetic patients of comparable age, gender, socioeconomic status, duration of diabetes, and comorbidity status. The average age of the 139 002 matched patients was 66, and of those who had taken a GLP-1 agonist, 97.5 per cent had used semaglutide.
Over the course of three years, 0.2 per cent - that's two per 1000 - of diabetic patients who took GLP-1 agonists developed neovascular AMD, compared to 0.1 per cent of those who did not. But this doubling of risk was only part of the story. Short-term use - 6 to 18 months - slightly reduced the chances of developing neovascular AMD, but those who had racked up 18 to 30 months of use had more than double the risk compared to nonusers, and those who kept taking a GLP-1 agonist for 30 months or longer had more than triple the risk. This dose-response effect is one of the signals that researchers use to identify a potential causal relationship between an exposure and a disease.
It's important to understand that a case-control study like this one cannot prove that GLP-1 agonists cause neovascular AMD; further research in other populations, including people using the drugs for weight loss rather than diabetes, is required. However, there are two plausible mechanisms of action for a causal relationship:
Firstly, GLP-1 agonists rapidly lower blood glucose level (which is why they're prescribed to diabetics). However, they may work so well that they cause hypoxia - low oxygen - in the retina of the eye. This oxygen deprivation drives the growth of new blood vessels, as a desperate workaround to try to meet the "exceptionally high oxygen demand" of this extremely energy-hungry tissue1.
Secondly, the retina itself contains GLP-1 receptors, and GLP-1 agonists increase the levels of several biochemicals that drive harmful blood vessel formation.
Interestingly, a study drawing from the TriNetX United States collaborative network, which aggregates deidentified electronic health record (EHR) data from 62 health care organisations, found that patients taking GLP-1 agonists had a reduced risk of the more common dry or nonexudative form of AMD compared with matched patients who were taking metformin, insulin, or a statin. In the case of neovascular AMD, however, GLP-1 agonist use was only associated with reduced risk when compared to insulin... and insulin use is a known risk factor for developing neovascular AMD!
Furthermore, only 9669 patients taking GLP-1 agonists were identified in this study, compared to the 46 334 in the Canadian study discussed above, and in retrospective cohort studies like these, size definitely matters.
On a personal note, I have a related but different form of macular degeneration called myopic macular degeneration, which occurs in people with high myopia (that's extreme shortsightedness, not the peculiar visual fixations that occur while smoking weed). Three years ago, completely out of the blue, the vision in my left eye became blurry. Distant telegraph poles no longer appeared as vertical lines, but as disjointed sections mysteriously suspended above each other in parallel. When I tried to read, letters and numbers danced before my eyes, before sliding into an invisible pit at the centre of my vision. It was, frankly, terrifying.
Fortunately I was able to get a prompt diagnosis and treatment by a skilled opthalmologist, which stabilised my condition. However, I still cannot see clearly out of my left eye, and I'm at high risk of experiencing another episode either in that eye, or the other one. It's not pleasant to live with the threat of becoming blind; I wouldn't wish it on anyone (OK, there are a few total scumbags that I might make an exception for, if I were pushed).
The whole idea that people with type 2 diabetes - a diet-and-lifestyle-induced condition that is completely reversible in most cases - are being put on drugs that could make them go blind, rather than being educated about the true causes of insulin resistance and receiving the support they need in order to turn it around, is just bonkers.
Speaking of bonkers, let's dig into the other study that I mentioned.
The miracle weight loss drug that makes you wish you were dead
I discussed the evidence for an increased risk of suicidal ideation in GLP-1 agonist users in The high price of weight loss: GLP-1 agonist side-effects:
"After reports to the Icelandic medicines agency of suicidal thoughts and self-injury in people using liraglutide and semaglutide, in July 2023 the Pharmacovigilance Risk Assessment Committee of the EMA launched a review of these harms in people taking any of the GLP-1 agonists. By this time, the EMA had retrieved 'about 150 reports of possible cases of self-injury and suicidal thoughts' for analysis. As of December 2023, the case reports had climbed to 'at least 170' and the EMA had requested more information from the pHarma companies that produce these drugs.
Meanwhile, by October 2023, the US Food and Drug Administration (FDA) had received 265 reports of suicidal thoughts or behaviour in people taking GLP-1 agonists, including 36 deaths by suicide or suspected suicide, since 2010. The news agency Reuters obtained 113 detailed narratives from these FDA reports. Here’s a taste of what they found:
“More than half of the narrative summaries describe suicidal thoughts appearing shortly after the person started the medicine or increased the dose. About two fifths of them said symptoms ceased after the patient stopped taking the drug or lowered the dose.
Thirty of the 113 narratives described patients with a history of depression, suicidal thinking or another mental-health condition. Another five reports explicitly said the patient had no history of psychological issues. Most reports don’t address that medical history.”
Wegovy, other weight-loss drugs scrutinized over reports of suicidal thoughts
In an analysis of 230 reports of suicidal events to the European Pharmacovigilance Database, published in February 2024, liraglutide had the highest reporting probability of suicidal ideation and suicide attempts, followed by semaglutide. Reporting probability was lower for dulaglutide and exenatide.
However, only liraglutide (Saxenda) carries an FDA warning for this adverse effect, because suicidal thoughts or behaviours were documented during the clinical trials used to gain regulatory approval for the drug. This takes ‘dying to lose weight’ to a whole new level."
OK, so some people develop suicidal thinking when they use GLP-1 agonists, but not all users do. In fact, the FDA issued a statement about the drugs in January 2024, reassuring the public that
"Our preliminary evaluation has not found evidence that use of these medicines causes suicidal thoughts or actions."
Given that these are the same people who told you that the COVID-19 injections were 'safe and effective' and would definitely prevent you from getting and spreading COVID, I'll leave it up to you to evaluate their trustworthiness.
What might explain the widely varying impact of these drugs on different individuals? Genetic variation between individuals is certainly part of the picture. There's an entire field of study called pharmacogenomics, which is defined as "the genomic profiling of patients for genetic variants that clinically modify the tolerability and desired effect of specific medications". In other words, any given drug is going to have fewer adverse effects and/or better therapeutic effects in some individuals than others, owing to gene variants that alter the metabolism of said drug. If you're really unlucky, you might have gene variants that cause you to get nasty side effects and little to no therapeutic effect. Bummer.
It turns out that GLP-1 agonists have a major influence on the dopamine pathway, which is a crucial element of the brain's reward circuitry. This reward circuitry drives eating behaviour, and in particular, the preference for foods high in fat and sugar. GLP-1 agonist users frequently report that the drug makes it easy for them to lose weight because they just aren't interested in food anymore - that is, they're not getting a reward response from it. Many report that soon after they start taking the drug, the "food noise" in their heads quiets down, for the first time in their lives that they can remember. This downregulation in reward signalling even transfers across to addictive disorders, with both anecdotal reports and limited clinical evidence finding decreased cravings for alcohol and cigarettes in people who use GLP-1 agonists, especially if they're also obese. Even shopaholics and obsessive nail pickers report relief from the obsessive thinking that drives their compulsive behaviours.
That's exciting news for those who suffer from substance and behavioural addictions, or attempt to help such sufferers, because they are notoriously refractory to treatment. However, the buzz around using GLP-1 agonists to treat addiction might be obscuring a poison pill: the very same mechanism that tamps down addictive processes - squelching dopamine signalling - can also induce depression and suicidal ideation (intrusive thoughts about killing oneself).
In a study conducted by an international team of researchers based in the US, South America, Israel and Iran2, advanced pharmacogenomic computational analyses were performed to identify genetic pathways that may induce depressive behaviour and suicidal ideation in individuals with particular genetic variants and epigenetic changes that have already led to reduced dopamine signalling.
They identified interactions between GLP-1 agonist drugs and 29 genes that code for the production of proteins involved in reward signalling, mood regulation, inflammation and cognitive function, with six genes being particularly affected. The researchers consulted three different databases that log associations between gene expression and disease conditions, and found that
"The most significant associated disease-causing phenotype among all three databases was major depressive disorder."
And wouldn't you know it, the same databases revealed that
"Depressive phenotypes and dopamine regulation are the most significant associated factors playing remarkable roles in SI [suicidal ideation]."
While the authors of the study acknowledge that their work is exploratory and theoretical, they also emphasise that its findings are supported by accumulating clinical evidence of new-onset depression and suicidal thinking in people who use GLP-1 agonists. They express alarm about the skyrocketing prescription rates of these drugs, for an ever-expanding range of clinical indications, and caution that long-term use is highly likely to seriously disturb dopamine signalling. In a significant proportion of patients, this disturbance will result in depression and suicidal ideation and unfortunately, a percentage of those people who keep thinking about killing themselves will eventually do it.
At a bare minimum, they advise screening patients for genotypes displaying low dopamine function before prescribing GLP-1 agonists. Yeah, good luck with that one, fellas.
They're not 'side effects', they're effects
Both of these unwanted consequences of the therapeutic mechanism of GLP-1 agonists are prime examples of what the pharmaceutical industry likes to call 'off-target' effects - that is, the biological activities of a drug that are not those of its intended biological target. GLP-1 agonists are intended to target GLP-1 receptors in the gut and brain in order to suppress appetite and slow down gastric emptying so that people eat less and hence lose weight. But there are GLP-1 receptors in the retina too, and they respond to the drug in an undesirable and - apparently - unanticipated way, potentially causing some people to go permanently blind. And the effect of GLP-1 receptor activation on dopamine signalling can make some people severely depressed to the point of actively wanting to die. Oopsie.
But as I wrote in Stop calling them ‘side effects’,
"There are no ‘side-effects’ of drugs. Every change that a drug causes is an effect. Some of those effects are desirable to doctor and patient; some are undesirable, but all result from interference with human physiology."
This message was drummed into me and my fellow naturopathy students over and over by our pharmacology lecturer, who also lectured medical students. And yet, astonishingly, researchers and doctors who know (or should know) about the 26 previous miracle weight loss drugs that were eventually taken off the market because they sickened, maimed and killed an unacceptably high proportion of the people who took them, somehow think that the GLP-1 agonists are going to be an exception to this rule. How is this selective amnesia cultivated in people with high IQs and (supposedly) good educations? I wish I knew.
But here's something I do know: the GLP-1 agonist freight train hasn't hit full speed yet. Novo Nordisk, the drugmaker behind semaglutide, is currently conducting a clinical trial to "look at how well semaglutide helps children and teenagers losing weight" (who writes this stuff???) and is enrolling children as young as six from all over the world. You'll be pleased to know that the study is designed to test the "long-term safety and efficacy" of the drug in this patient population, and by long term, they mean.... two and a half years. That's kind of convenient, given that previous research conducted in adults concluded that weight loss plateaus in the second year of use (which could be a good thing in children given that you don't want them to keep on losing weight indefinitely while they're actively growing) and that adverse effects such as the macular degeneration, depression and suicidal ideation documented in the two studies I discussed above, may take longer than 30 months to show up, especially in children.
And let's be crystal clear about something: the companies that make GLP-1 agonists know that once people get started on these drugs, they have to keep taking them long-term - perhaps, for the rest of their lives - because rebound weight gain occurs as soon as people stop using them. I don't even know what to say to parents who would enrol their precious child in this clinical trial. You might as well just cut out the middle-man and sacrifice them straight to Moloch. I totally understand that we live in an obesigenic environment but come on, people - how could you possibly think that injecting your child with a drug that alters their biochemistry in a fundamental and potentially permanent way, is the right solution? And what the hell does it say about our societies, that we shrug our collective shoulders about this atrocity being perpetrated on our children?
Anyway... I know that 99.9999 per cent of my readers are as flabbergasted as I am by the GLP-1 agonist major-tragedy-just-waiting-to-happen, so here's what I'd like you to do: Share this article with someone you know, who is battling their weight or struggling to get their diabetes under control, and has been advised to take a GLP-1 agonist. Or - god forbid - someone you know who is already using one of these drugs. And if you happen to know anyone who has already, or is considering, enrolling their child in that clinical trial, please phone child protective services immediately. Just kidding... or maybe not.
Last thing: This post took me approximately 15 hours to research and write. If you feel you’ve gotten value from it, please consider a paid subscription to help me continue this work:
For information on my private practice, please visit Empower Total Health. I am a Certified Lifestyle Medicine Practitioner, with an ND, GDCouns, BHSc(Hons) and Fellowship of the Australasian Society of Lifestyle Medicine.
A related process - angiogenesis - occurs in the oxygen-starved centre of malignant tumours. The difference between neovascularisation and angiogenesis is that in angiogenesis, new blood vessels form from previously existing blood vessels, while in vasculogenesis, vessels arise from cells that are not meant to be blood vessels; and neovascularisation combines both of these ways of developing new blood vessels.
Fancy that! There are actually Iranians who aren't crazed Jew-hating apocalyptic death-cult Islamists chanting 'Death to America! Death to Israel!' Maybe we shouldn't go and bomb the bejeezus out of their country after all. </sarcasm>