


Why Australia’s COVID-19 exit plan can’t succeed
Part 2

In last week’s post, I laid out the evidence that the currently-available experimental COVID-19 injections (including the Pfizer, AstraZeneca, Janssen-Cilag/Johnson & Johnson and Moderna shots granted provisional registration in Australia) do not prevent infection with and transmission of SARS-CoV-2, the virus associated with COVID-19, and therefore cannot achieve herd immunity.
In this week’s post, I will present evidence that these experimental injections are more than likely responsible for the development of new variants of SARS-CoV-2 that are resistant to any ‘immunity’ they may confer; and that they may be sowing the seeds for a devastating wave of serious illness thanks to vaccine-induced escape mutants and antibody-dependent enhancement.
Development of SARS-CoV-2 “variants of concerns” linked to use of ‘vaccines’
Mutation – that is, a change in the DNA or RNA sequence of the genome – is simply the order of the day for viruses, as it is for all other life forms:
“Mutations are the building blocks of most of evolution—they are the variation upon which natural selection can act, and they are the cause of much of the novelty we see occur in evolution.”
Most mutations are harmful to the organism or biological entity that they occur in, causing them to be naturally selected out. Many are inconsequential, allowing them to persist. A small percentage of mutations confer a survival benefit to the organism or biological entity, causing them to become dominant over others of their kind, over the course of time.
The difference between mutation rates in animals – including humans – and mutation rates in viruses, of course, is that viruses reproduce themselves far more rapidly than their living hosts.
Viruses are non-living, and can only replicate themselves by gaining entry into the living cells of organisms and hijacking their cellular machinery on order to make more copies of themselves. Every time they replicate, one or more mutations can occur.
This rapid mutation rate allows viruses to adapt to conditions within an individual host with incredible speed, and also to refine their ability to transmit between hosts more efficiently:
“RNA viruses [including SARS-CoV-2, although coronaviruses are generally more genetically stable than most RNA viruses] have high mutation rates—up to a million times higher than their hosts—and these high rates are correlated with enhanced virulence and evolvability, traits considered beneficial for viruses.”
So the fact that variants of SARS-CoV-2 have emerged is not at all surprising; it’s virology 101.
The World Health Organisation (WHO) and its partner agencies have been tracking the evolution of variants of SARS-CoV-2 since January 2020.
However, WHO only began designating some of these as “variants of concern” – that is, variants with increased transmissibility and/or virulence (disease-causing capacity) and/or resistance to vaccines or treatments – in mid-December 2020, coinciding with the beginning of the ‘vaccine’ rollout in Western countries.
Comparing the location of ‘vaccine’ trials – in which tens of thousands of volunteers were administered the experimental injections – with the locations in which variants of concern were first documented, reveals a pattern which is, to say the least, very interesting:
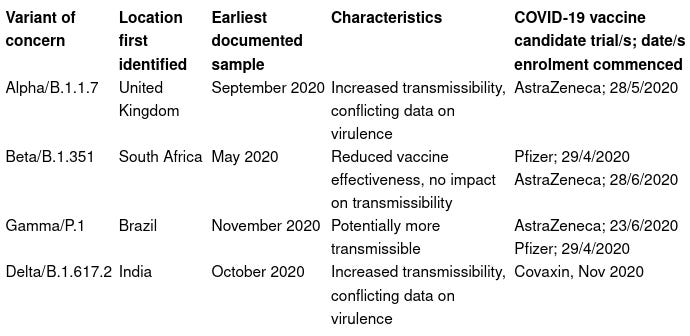
In other words, variants of concern emerged in all three countries which hosted phase 3 trials of the AstraZeneca injection, and two out of the six countries in which phase 3 trials of the Pfizer product were conducted. (The Iota “variant of interest” was also first identified in the US, which hosted trials of the Pfizer and Moderna shots, in November 2020.)
The fact that vaccination drives the development of viral variants is well established, and was freely discussed by virologists in the years BC (Before COVID-19):
“A vaccine is a novel selection pressure placed on a pathogen, and if the vaccine does not eradicate its target completely, then the remaining pathogens with the greatest fitness — those able to survive, somehow, in an immunized world — will become more common.”
But in addition to the natural evolutionary process by which random mutations in viruses gradually reduce the effectiveness of most vaccines over time, so-called “imperfect vaccines” or “leaky vaccines” – vaccines which reduce pathogen growth rate and/or toxicity but do not block infection – actually select for mutations that make viruses vaccine-resistant:

Vaccines Are Pushing Pathogens to Evolve
“Leaky” vaccines drive the development of more deadly variants
It’s not just vaccine resistance that is selected for by “leaky vaccines” such as COVID-19 jabs. More worryingly still, leaky vaccines are known to drive the development of more virulent variants, resulting in more severe illness and death:
“The subsequent evolution leads to higher levels of intrinsic virulence and hence to more severe disease in unvaccinated individuals. This evolution can erode any population-wide benefits such that overall mortality rates are unaffected, or even increase, with the level of vaccination coverage.”
The COVID-19 ‘vaccines’ currently available are all leaky vaccines, as I showed in Part 1. And researchers are now beginning to grapple with the question of whether ‘vaccinated’ individuals are indeed driving the development of SARS-CoV-2 variants that evade existing COVID ‘vaccines’.
A study published on 30 July 2021 in Scientific Reports drew the following conclusions:
“The coincidence of a high number of vaccinated individuals and a high rate of transmission has two effects on the resistant strain. First… because the rate of transmission is high, the emerging resistant strain is not lost through genetic drift… Second, a high number of vaccinations creates a selective advantage of the resistant strain over the wildtype strain…
The highest risk of resistant strain establishment occurs when a large fraction of the population has already been vaccinated but the transmission is not controlled.”
Rates of SARS-CoV-2 transmission and vaccination impact the fate of vaccine-resistant strains
And it’s just this scenario – large fraction of the population ‘vaccinated’, but uncontrolled transmission of the virus – which we are seeing now in the UK, US, Israel, Chile and Mongolia, among others.
As the US Centers for Disease Control and Prevention (CDC), admits, the Delta variant, which is now responsible for 80% of COVID-19 cases in the US for which genomic sequencing is available, can be transmitted just as readily by ‘vaccinated’ as by unvaccinated people.
In other words, it’s not the unvaccinated that are the “human petri dishes” brewing up potentially dangerous viral variants, it’s the ‘vaccinated’.
The much-touted ability of COVID-19 vaccines to reduce serious illness and death (if true, which is somewhat dubious), without preventing infection or transmission, creates the perfect storm scenario in which the virus continues multiplying within its host, mutating as it does so, and in the process “learning” how to evade the host’s incomplete immune response.
The mutations it thus acquires allow it to “evolve to become deadlier to unvaccinated hosts because it can reap the benefits of virulence without the costs.”
“Anti-disease vaccines that do not prevent transmission can create conditions that promote the emergence of pathogen strains that cause more severe disease in unvaccinated hosts.”
Imperfect Vaccination Can Enhance the Transmission of Highly Virulent Pathogens
But don’t think for one moment that it’s only those who can’t or won’t receive a COVID-19 jab that may be adversely affected by this vaccine-generated “hot” variant:
“This virulence can also cause the vaccine to start failing by causing illness in vaccinated hosts.”
And that’s exactly what the CDC’s analysis of the outbreak in Barnstable County, Massachusetts showed: 79% of the ‘fully vaccinated’ patients who became infected were symptomatic, and 4 of the 5 patients who had to be hospitalised were ‘fully vaccinated’.
Antigenic sin
“Antigenic sin” occurs when a vaccine generates antibodies to the particular strain of the virus used in the vaccine, but the person subsequently encounters a variant of the virus that is not neutralised by the vaccine-induced antibodies.
When people contract an infection, the natural immunity that they develop generally gives them durable protection, including to variants, because natural immunity results in antibodies to the entire surface of the virus, not just one element of it. In addition, natural immunity results in the development of T cells which combat the virus before it even encounters any antibodies.
In contrast, mRNA and viral vector COVID-19 injections are designed to elicit antibodies against only the spike protein of SARS-CoV-2, which just happens to be the part of the virus which is most rapidly mutating.
In antigenic sin, the vaccinated person’s immune response is so dominated by the vaccine strain of the virus that they can neither generate their own antibodies against the new variant, nor have those antibodies induced by a revaccination.
The consequences of antigenic sin are either anergy - a lack of immune response to the variant, resulting in persistent infection - or antibody-dependent enhancement - in which vaccine-induced antibodies, instead of preventing the virus from entering cells, paradoxically draw viruses into cells, facilitating infection and provoking a dangerous cytokine storm.
The UK’s Scientific Advisory Group for Emergencies (SAGE) claims that antigenic sin is a “less likely” scenario and that it has not yet been observed in COVID-19, yet the susceptibility of ‘vaccinated’ individuals to becoming infected with, and ill from, the Delta strain could indicate that it is indeed already happening.
Aside from the Barnstable County incident mentioned above, and described more fully in last week's post, the recent report that 14 Israelis were diagnosed with COVID-19 just one week after receiving a third injection of the Pfizer jab (a so-called "booster shot"), with two requiring hospitalisation for treatment, points toward the possibility that vaccines that induce antibodies against the original Wuhan strain of SARS-CoV-2 leave people incapable of mounting an immune response against variants with substantial genomic differences, such as the now-dominant Delta strain.
As for antibody-dependent enhancement, a phenomenon that plagued the development of previous coronavirus vaccines, a recently-published study demonstrated that vaccine-induced neutralising antibodies (the kind you want) have a decreased affinity for the spike protein of the Delta variant, while infection-enhancing antibodies (the kind you don’t want) have an increased affinity - in other words, the perfect set-up for antibody-dependent enhancement.
There are concerning signs that antibody-dependent enhancement may indeed be emerging in people who have received COVID-19 'vaccines':

Summing up
The current crop of COVID-19 injections do not stop infection with, or transmission of, SARS-CoV-2, are not capable of generating herd immunity; are almost certainly driving the development of more transmissible and possibly more virulent variants that sicken both the unvaccinated and the vaccinated; and hold the potential to unleash catastrophic consequences on the vaccinated through antigenic sin and antibody-dependent enhancement.
Universal uptake of these poorly-tested experimental products is not the solution to the manufactured “COVID crisis”. Returning to time-honoured policies of reducing exposure risk to the vulnerable, instructing people with symptoms to self-isolate, and allowing everyone else to go about their lives, along with implementation of evidence-based prophylaxis and treatment strategies for those who desire or require them, is the only tenable solution. And it has been right from the start.