


There must be fifty ways to leave your little people (dead, disabled or injured, that is)
(With apologies to Paul Simon)

In last week's post, The Great Australian Die-Off, I discussed the alarming increase in excess mortality - deaths above the expected level, in a given population over a given time-period - that has occurred in Australia since the roll-out of the experimental RNA transfection agents (falsely marketed to the public as 'vaccines') began.
As I noted in that article, there was no excess mortality in Australia in the pre-injection phase of the declared COVID-19 pandemic. Furthermore, Neil and Fenton's analysis of data from around the world indicates that neither COVID itself, nor long COVID, nor lockdowns, nor rationing of healthcare services, can explain the excess mortality seen in the 30-odd countries for which they could obtain adequate data on each variable. I strongly encourage you to read their article The Devil's Advocate: An Exploratory Analysis of 2022 Excess Mortality before continuing on, as it neatly dispenses with the pathetic (non)explanations for excess mortality that the legacy media have vomited up in service of their corporate masters, such as this pathetic waste of cybercharacters from that former bastion of journalistic integrity, the Sydney Morning Herald, or this piece of scintillating stenography ("We asked the TGA if the jabs are killing people, and they said 'Nah, course not!'") from the Canberra Weekly, or this remarkably fact-free 'fact check' from the Trusted News Initiative's bottom-shelf whore, the ABC.
Of course, the fact that jab-happy nations are racking up excess mortality whereas largely unjabbed Africa has shrugged off COVID while racking up lower excess mortality than Eurasia and the Americas, does not prove that the experimental transfection agents are responsible for the unexpected deaths. As I discussed in If the COVID-19 injections work, why are more people dying? Part 2, the Bradford Hill criteria, otherwise known as Hill’s Criteria for Causality, are used to distinguish causal from non-causal associations between phenomena. Here are those criteria:
Strength of association – The stronger the association, the more likely it is that the relation is causal.
Temporal relationship – Exposure always precedes the outcome.
Consistency – The association is consistent when results are replicated with different people under different circumstances and with different measurement instruments.
Theoretical plausibility – It is easier to accept an association as causal when there is a rational and theoretical basis for such a conclusion.
Coherence – The association should be compatible with existing theory, hypotheses, and knowledge.
Specificity – In the ideal situation, the effect has only one cause. (In practice, an effect may have multiple contributing causes; for example, a genetic predisposition to lung cancer may combine with cigarette smoking and low intake of cancer-preventing nutrients to result in lung cancer.)
Dose response relationship – An increasing amount of exposure increases the risk.
Experimental evidence – Any related research that is based on experiments will make a causal inference more plausible.
Analogy – Sometimes a commonly accepted phenomenon in one area can be applied to another area.
Back when I wrote that article, far less was known about biologically plausible mechanism/s by which the transfection agents could cause injury and death, which are required to fulfil criterion #4. In the ensuing year, many scientific papers have been published (and many more yet-to-be-published papers have been uploaded to preprint servers) which elucidate those mechanisms. No doubt more will become evident in the months to years to come, so I will update this post as new information comes in.
Importantly, the accumulating body of evidence on mechanisms of harm dispenses with the hand-waving arguments quoted in the 'RMIT ABC Fact Check', namely that the excess non-COVID deaths couldn't possibly have been caused by the safe-and-effective™ vaccines, because they were attributed to dementia, cancer, ischaemic heart disease, cerebrovascular diseases, and infectious diseases other than COVID... and as for the historically unprecedented number of deaths attributed to "unspecified diseases", the Australian Actuaries Institute's spokesmuppet Karen Cutter dismisses these with the air-headed claim that "this is a large 'catch-all' category" from which it is difficult to draw conclusions. Well, yeah, it's very difficult to draw conclusions about whether someone's death was caused by an RNA transfection agent if you don't utilise the correct procedures during autopsy, or you don't autopsy them at all.
(For detailed presentations on how to detect spike protein generated by the transfection agents and the immune reaction to them during autopsy, and how to distinguish this from the effects of infection with SARS-CoV-2, watch the videos on this page.)
Mechanism #1: Impaired immune function
By now, many people have seen the following graph, from a study of Cleveland Clinic healthcare workers, which shows a clear dose-response relationship between COVID-19 shots and the risk of getting COVID - that is, the more injections, the more infections:
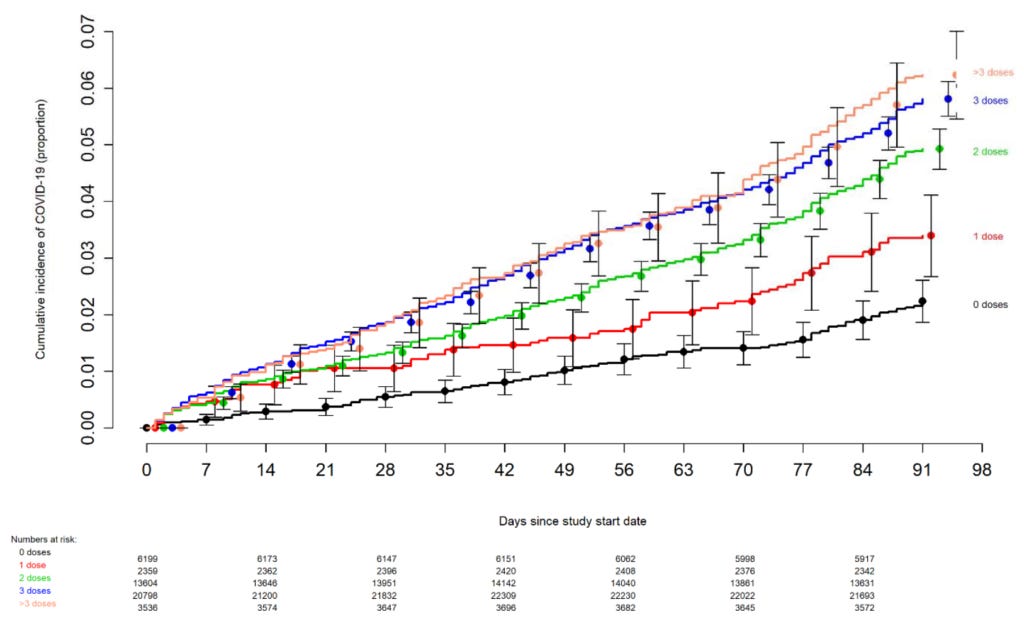
The Cleveland Clinic study confirms many people's anecdotal observations that their multiply-jabbed friends are not just 'getting COVID' (whatever that means) every second Tuesday; they're also picking up all manner of other infections. Meanwhile, those who either decided against receiving any experimental injections, or called it quits after the initial series, are remaining remarkably unscathed.
Several papers elucidating mechanisms of immune suppression that could explain these phenomena have been published:
A seminal paper published in March 2022, 'Immune imprinting, breadth of variant recognition, and germinal center response in human SARS-CoV-2 infection and vaccination' found that people who got infected with SARS-CoV-2 initially mounted an immune response tailored to the particular variant that infected them, and then developed a broad immunological response to viral variants, over several months post-infection. However, the immune systems of people who had received an mRNA transfection agent were 'locked in' to producing useless antibodies against the original but now extinct Wuhan variant of SARS-CoV-2, rendering them susceptible to being reinfected over and over again with new variants of the virus. These reinfections repeatedly expose them to the hazards of the virus' spike protein. And, even worse, both mRNA from the experimental injections, and spike protein stimulated by them, was found in the germinal centres of lymph nodes for up to two months post-injection (after which testing stopped).
An article published in June 2022, titled 'Innate immune suppression by SARS-CoV-2 mRNA vaccinations: The role of G-quadruplexes, exosomes, and MicroRNAs' reports that the mRNA transfection agents suppress type 1 interferon response, resulting in impairment of innate immunity, the body's first-line defence against both viruses and bacteria. In other words, impaired innate immunity increases susceptibility not just to repeated bouts of COVID-19, but to other infectious agents such as RSV, influenza and strep A. That 'tripledemic' of flu, COVID and RSV that the mockingbird media have been incessantly squawking about, may well have been brought on by suppression of type 1 interferon, as may the disappearance of viral interference that held flu and RSV in check when SARS-CoV-2 first emerged.
The immune system's ability to suppress the herpes zoster virus is also impaired by RNA transfection agents. Herpes zoster virus causes chickenpox on first exposure, and then reverts to a latent form inside nerve cells. Immune suppression can trigger it to reemerge in later life as shingles. Not only can shingles itself be fatal, especially in older age groups, but it is also associated with a higher long‐term risk of a major cardiovascular event. In August 2022, an article titled 'Real-world evidence from over one million COVID-19 vaccinations is consistent with reactivation of the varicella-zoster virus' found an 80 per cent higher risk of developing shingles in people who had received a COVID-19 injection.
A preprint posted in September 2022, 'Correlates of protection, viral load trajectories and symptoms in BA.1, BA.1.1 and BA.2 breakthrough infections in triple vaccinated healthcare workers', notes that 22 per cent of 368 Swedish healthcare workers developed an infection with the Omicron variant within 4 weeks of receiving an mRNA booster, and that most participants had a persistently high viral load and showed delayed clearance of the virus, indicating not only that their immune system was struggling to vanquish it, but also that they were still infectious for up to 9 days after first testing positive on qPCR.
To summarise, a growing body of evidence shows that COVID-19 transfection agents impair immune function in ways that increase susceptibility to infection with SARS-CoV-2 and other viruses, and decrease the immune system's ability to suppress latent viruses. Those who wish to argue that the excess deaths seen in Australia and overseas are at least partly due to after-effects of COVID-19, and to the reemergence of influenza, need to reckon with the fact that the transfection agents are causing people to become repeatedly reinfected with SARS-CoV-2 and to be more susceptible to infection with other viruses.
Mechanism #2: Extensive damage to the cardiovascular system
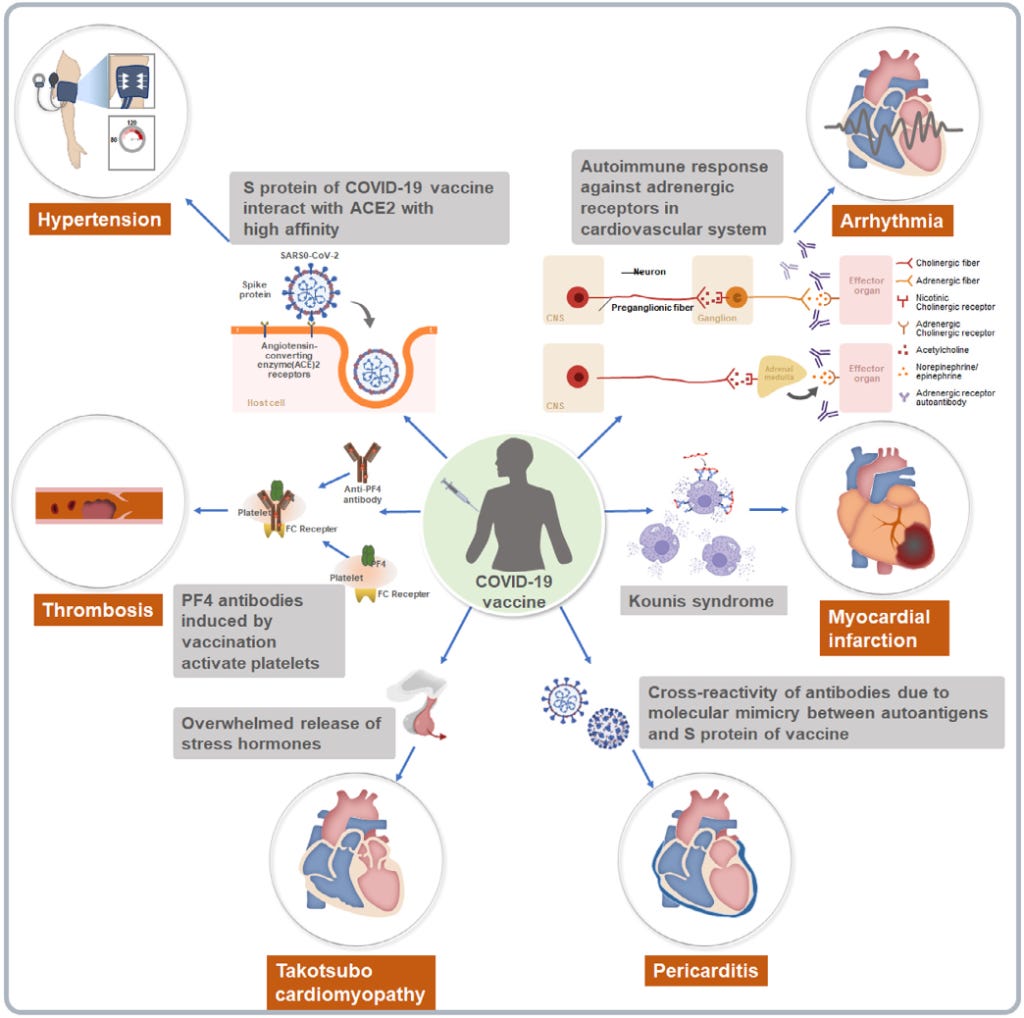
A review article published in November 2022, 'Clinical cardiovascular emergencies and the cellular basis of COVID-19 vaccination: from dream to reality?', sifted through data from published case reports, studies and pharmacovigilance databases to compile a comprehensive list of adverse effects of the experimental transfection agents on the heart, blood vessels and cellular components of blood.
These damaging impacts include:
Incitement of pro-inflammatory immune cells, and/or generation of self-antibodies (i..e. an autoimmune reaction) to cells of the heart muscle and the fluid-filled sac that surrounds it, leading to myocarditis and pericarditis. Myocarditis may lead to cardiac arrest (the sudden loss of all heart activity due to an irregular heart rhythm).
Abnormal clotting, with or without depletion of platelets (thrombosis and thrombocytopenia), through induction of antibodies against clotting factors and inflammatory cytokines, platelet activation and aggregation, increased vascular permeability (blood vessel leakiness) and activation of the endothelial cells that line blood vessels. Thrombotic events can also lead to heart attacks and strokes.
Interaction of spike protein generated by the transfection agents with ACE2 receptors, causing hypertensive crisis (sudden and dramatic elevation of blood pressure).
Hypersensitivity reactions to excipients (substances other than the active drug), leading to Kounis syndrome, an acute coronary syndrome in which a severe allergic response shuts down blood supply to the heart muscle, by causing coronary vessels to go into spasm, atherosclerotic plaque to abruptly erode, and stents to occlude (block up) with mast cells and/or eosinophils (types of white blood cells). This constellation of pathologies can lead to a myocardial infarction (heart attack).
Induction of arrhythmias (abnormal health rhythms) including tachycardia, atrial fibrillation, sinus tachycardia, and supraventricular tachycardia, along with postural orthostatic tachycardia syndrome (POTS). One potential cause of these arrhythmias is an autoimmune response against adrenergic receptors in the cardiovascular system.
A systemic inflammatory reaction that sensitises patients to catecholamines (acute stress hormones), leading to Takotsubo cardiomyopathy. Also known as stress cardiomyopathy or, more colloquially, 'broken heart syndrome', this condition manifests in a sudden temporary weakening of the muscular portion of the heart. It confers a nearly 10 per cent risk of major cardiac events (such as heart attack, stroke and heart failure) and a 5.6 per cent patient mortality rate per year.
The authors even provided a handy-dandy chart summarising all the fun and exciting ways that the experimental transfection agents can damage your cardiovascular system:
At the end of their discussion of the transfection agents' association with cardiac arrest and death, the authors make a summary statement which you should read several times, slowly, to let it sink in:
"Given the observed mortality, recommendations for vaccination in the elderly (aged >80 years) should be reconsidered. In patients with multimorbidity in a suboptimal situation before vaccination, vaccine-drug and vaccine-disease interactions in polypharmacy users might have contributed to worsened health outcomes (Qamar et al., 2022). The general vaccination response and potential immune stimulation might be sufficient to trigger decompensation of underlying diseases and prompt death (Thomas et al., 2021)."
In other words, the people whom we're told are in gravest need of the experimental transfection agents, because they are at the highest risk of a severe outcome of SARS-CoV-2 infection, are also at the highest risk of being fatally injured by the jabs. Do you see now how utterly duplicitous it is for Professor Tom Marwick, director of the Baker Heart and Diabetes Institute, to wave away the excess deaths as just an escalation of a preexisting burden of cardiovascular risk factors, or for the Australian Actuaries Institute's Karen Cutter to insist that the injections couldn't possibly be causing excess deaths because most of those deaths are occurring in the elderly, whereas the majority of young and middle-aged adults got jabbed too?
Even if one accepts their argument that COVID-19 itself is causing increased cardiovascular deaths because of the damaging effects of the SARS-CoV-2 spike protein on the heart and blood vessels, let's remember that the risk of infection with currently-circulating strains of the virus is increased, in a stepwise fashion, the more jabs one submits to. Whichever way you try to slice and dice it, either directly or indirectly the injections are causing excess cardiovascular deaths.
Mechanism #3: Impaired synthesis of regulatory proteins
The authors of the previously cited paper 'Innate immune suppression by SARS-CoV-2 mRNA vaccinations: The role of G-quadruplexes, exosomes, and MicroRNAs' also noted that they have identified "potential profound disturbances in regulatory control of protein synthesis and cancer surveillance" triggered by the large amounts of spike protein production induced by the injections. These disturbances could "potentially have a causal link to neurodegenerative disease, myocarditis, immune thrombocytopenia, Bell's palsy, liver disease, impaired adaptive immunity, impaired DNA damage response and tumorigenesis."
In other words, by messing with the body's normal patterns of response to infection, the mRNA injections set off a cascade of harmful effects that ripples throughout virtually every system of the body. But is there evidence that this is indeed happening? The authors found an unprecedentedly high number of reports of each condition mentioned above in the Vaccine Adverse Events Reporting System (VAERS), the US vaccine pharmacovigilance tool.
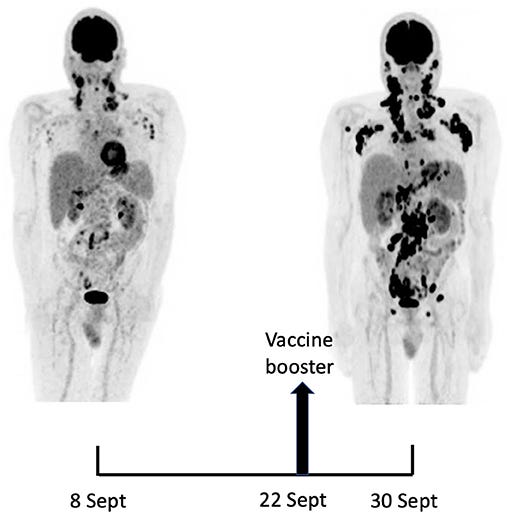
In addition, case reports of these types of injuries are increasingly appearing in the medical literature, such as this report of a 60 year old doctor who developed lymphoma in his left cervical lymph nodes five months after completing his primary series of Pfizer transfection agents in his left deltoid muscle, only to experience rapid development of cancerous lesions in his right armpit and neck, within eight days of receiving a Pfizer booster in his right deltoid:
Conclusion
The Therapeutic Goods Administration (TGA) asserts that it is "false and unscientific to automatically conclude that vaccines caused these [excess] deaths". I agree. Each unexpected death should be thoroughly investigated by unbiased experts, rather than being airily dismissed as 'Sudden Adult Death Syndrome', which we're now all supposed to believe is incredibly common; somehow we just didn't notice before that perfectly healthy young and middle-aged people were abruptly dropping dead in the midst of their daily activities, or going to sleep and never waking up. (See Mark Crispin Miller's Substack for a gut-wrenching weekly compendium of reports of these ‘died suddenly’ deaths from all over the world.)
Subject to permission of the deceased's family, an autopsy should be conducted on each of these deaths, using the protocol developed by experienced German pathologist, Dr Arne Burkhardt. This protocol includes immunohistochemistry to detect the spike and nucleocapsid proteins of SARS-CoV-2 (which distinguishes infection from inoculation as a cause of death), and to detect infiltration of tissues by specific immune cells that respond to components of the injections.
When the TGA insists that "There is no credible evidence to suggest that COVID-19 vaccines have contributed to excess deaths in Australia or overseas", I can only assume that they are, like Admiral Nelson, holding the telescope up to their blind eye. Nelson's recklessness won battles; the TGA's is costing thousands of Australian lives.
Despite all the obfuscation, misdirection and outright lying of the government, its media mouthpieces and even trade associations like the Australian Actuaries Institute, there are far more proven mechanisms by which the COVID-19 transfection agents damage, disable and kill, than ways that Paul Simon came up with for leaving your lover:
You just slip out the back, Jack
Make a new plan, Stan
You don't need to be coy, Roy
Just get yourself free
Oh, you hop on the bus, Gus
You don't need to discuss much
Just drop off the key, Lee
And get yourself free
Slip out the back, Jack
Make a new plan, Stan
You don't need to be coy, Roy
You just listen to me
Hop on the bus, Gus
You don't need to discuss much
Just drop off the key, Lee
And get yourself free
The fact that the agency charged with ensuring that the medicines Australians take are safe and effective shows no interest whatsoever in investigating the historically unprecedented tsunami of injuries and deaths that has occurred since the 'vaccine' roll-out began, speaks volumes on whom they really serve.
The credible evidence they claim doesn't exist also includes actuarial data, insurance data, coroner reports, trial data, admissions of fraud under oath, court rulings, submissions addressed directly to them from groups of honest doctors, and death as, literally, a listed side-effect. Traditionally, less credible evidence is anecdotal, however with such widespread corruption in this 5g warfare, particularly of 'science', i argue that anecdotal evidence is currently gold standard.
This post is outstanding. The excellent summary of the many ways the experimental Covid-19 injections cause disease and death is especially illuminating -- and very helpful to have captured in one place. Thank you for your excellent work!