


The perils of proton pump inhibitors - Part 2
Are PPIs really as safe as we've been led to believe?

In Part 1 of this series on proton pump inhibitors, I covered the basics - how these drugs work, what they're supposed to be prescribed for, and the deeply concerning rate of inappropriate use of these medications.
And now, in Part 2, I'll examine the known and suspected adverse effects of PPIs, and why they might occur.
PPIs: The risks
Medical authorities generally consider PPIs to be safe when used for brief periods, despite mounting evidence that they induce adverse changes in the gut microbiota, which in turn increase the risk of a host of maladies (more on that, shortly).
But even the staunchest defenders of PPIs acknowledge that the risk of serious side effects associated with their use rises, the longer people stay on them. These serious adverse outcomes include:
1. Pneumonia
Even short-term use of PPIs increases the risk of pneumonia (both community- and hospital-acquired) by up to 39 per cent. High-dose PPI therapy, and taking more than one dose per day, increase the risk more than low-dose and single-dose-per-day therapy.
2. Clostridioides difficile infection
Formerly known as Clostridium difficile, Clostridioides difficile (C. diff) is a bacterium that can infect the bowel. If you have a mild case of C. diff infection, you'll suffer diarrhoea and stomach cramping that resolves in a matter of days. But in severe cases, C. diff can cause colitis, which results in copious, bloody diarrhoea, violent cramping, fever, nausea, loss of appetite, severe dehydration and rapid heart rate. Rare but life-threatening complications of C. diff infection include sepsis, toxic megacolon, and perforation of the bowel leading to peritonitis.
C. diff infections commonly occur after taking antibiotics, probably because these medications disrupt the gut microbiota. Clindamycin, fluoroquinolones, penicillin beta-lactamase inhibitor combinations, amoxycillin and broad-spectrum cephalosporins are particularly strongly linked to C. diff infection, but any antibiotic can precipitate this potentially life-threatening bacterial overgrowth.
Given that stomach acid suppresses the growth of bacteria, it should come as no surprise that C. diff infection is more than twice as likely to occur in people who are taking PPIs. As with pneumonia, the risk rises with higher doses, and taking more than one dose per day.
3. Other dysbiotic conditions
Even short-term use of PPIs increases the risk of manifestations of dysbiosis (gut bacterial imbalance) other than C. diff infection. These include:
Small intestinal bacterial overgrowth, a common cause of IBS-type symptoms such as bloating, diarrhoea and/or constipation;
Spontaneous bacterial peritonitis, an abnormal accumulation of bacteria-infected fluid in the abdomen;
Hepatic encephalopathy, impaired brain function occurring in patients with advanced liver diseases, which can be caused by excess ammonia-producing gut bacteria; and
Adverse outcomes in inflammatory bowel disease (Crohn's disease and ulcerative colitis).
Worse yet, PPI use increases the risk that your intestine will be colonised with multidrug-resistant microorganisms such as vancomycin-resistant enterococci, by 75 per cent. In other words, if you do develop a serious dysbiotic condition, it's less likely to be treatable with any currently-available antibiotic. And that means you'll be more likely to die from your infection.
4. Viral gastroenteritis
Just like respiratory viruses, enteric viruses that are associated with acute gastroenteritis of viral origin ('stomach flu') reach their peak of activity during winter. In a study of over 860,000 French people, just over a quarter of whom were regularly taking PPIs, the risk of stomach flu was found to be 1.8 times higher in people who were taking a PPI. For people aged 65 to 74 years, continuous PPI therapy more than doubled the risk.
5. Bone fractures
Overall fracture risk is heightened in people taking PPIs, and in particular, hip and spinal fractures have been found to be associated with their use. Higher doses and longer duration of use increase the risk. A prospective trial of 1211 postmenopausal women found that those taking omeprazole had 3.5 times the risk of suffering a vertebral fracture as nonusers, while a recent meta-analysis found a 26 per cent increased risk of hip fracture, after adjustment for calcium intake and duration of PPI use.
Even low dose PPI therapy increases hip fracture risk, but the risk escalates with higher doses. Surprisingly, there was little difference in fracture risk between short-term and long-term users.
6. Heart attack and stroke
PPIs substantially increase the risk of having a first myocardial infarction (heart attack) or a ischaemic (clotting) stroke, especially in people who take them at high doses and/or for long periods of time. Long-term use may increase the risk of ischaemic stroke by 29 per cent, and the risk of heart attack by 36 per cent. High dose users have a 31 per cent higher risk of stroke, and 43 per cent higher risk of heart attack than non users.
7. Acute and chronic kidney disease
The risk of chronic kidney disease is 50% higher in PPI users, especially in those taking multiple daily doses. And an analysis of data on over 208,000 Chinese patients admitted to an intensive care unit with sepsis (the body's overwhelming and life-threatening response to infection that can lead to tissue damage, organ failure, and death) found that long-term use of PPIs (and also H2 blockers, an older and weaker class of acid-suppressing drugs) was associated with higher mortality in septic patients with chronic kidney disease.
In a population-based study of Canadian adults aged 66 and over, PPI use increased the risk of acute kidney injury and acute interstitial nephritis by 2.5 and 3-fold respectively.
8. Gastric (stomach) cancer
Although the whole purpose of eradicating H. pylori using PPIs and antibiotics is to reduce the risk of gastric cancer, continuing to use a PPI long-term after eradication therapy may increase the risk of developing cancer of the stomach. Using a PPI for more than a year after H. pylori eradication increased gastric cancer risk by 5-fold; more than 2 years by nearly 7-fold; and more than 3 years by over 8-fold.
9. Depression, including major depressive disorder
A nationwide, retrospective population-based study conducted in Taiwan found that PPI use was associated with major depressive disorder; once again, higher doses and longer duration of use were associated with greater risk. Pantoprazole, lansoprazole and rabeprazole were more strongly associated with depression than omeprazole and esomeprazole.
10. Obesity
In a a cohort study of over 300,000 children with parents in the US military, those who were given PPIs in the first 2 years of life were found to be more likely to become obese, especially with longer duration of use, and in conjunction with antibiotics.
11. Allergic diseases
The same cohort study which found a link between PPI use and obesity, also studied allergic disease in almost 800,000 US children with a birth medical record in the Military Health System database. This study found that food allergy, anaphylaxis, asthma, atopic dermatitis, allergic rhinitis, allergic conjunctivitis, urticaria, contact dermatitis and medication allergies were more likely to develop in children who were given a PPI in the first 6 months of life.
In a nationwide cohort study which used registry data collected in Sweden, children aged 17 and under who used PPIs were found to be 57 per cent more likely to develop asthma. The risk was highest in the youngest children: infants aged under 6 months had an 83 per cent higher risk of asthma if they were administered a PPI, while toddlers aged 6 months to 2 years had a 91 per cent higher risk.
An analysis of data from health insurance records covering 97 per cent of the Austrian population found that PPI use in adulthood also increases the prevalence of allergic symptoms, particularly in older individuals and women.
12. Nutritional deficiencies
The efficient absorption of many nutrients, including iron, calcium and vitamin B12, is dependent on the presence of acid in the stomach. Deficiencies of iron and vitamin B12 have been reported in PPI users, while the increased risk of bone fracture discussed above indicates interference with calcium absorption and metabolism.
There are also many case reports and case series of PPI-induced hypomagnesemia (low levels of magnesium in the blood), which can induce seizures, cardiac events and tremors.
(Unlucky) 13. Increased risk of death
The ultimate adverse medication event is death. In a large-scale study of US veterans, the all-cause mortality rate of people taking a PPI was found to be 15 per cent higher than those taking H2 blockers, and 23 per cent higher than those taking no acid-suppressing medications at all. Longer duration of use was associated with increased risk of death.
How PPIs cause harm
As I emphasised in Stop calling them ‘side effects’, everything that a drug does to living cells, tissues and organs is an 'effect'. It's just that some of those effects are desirable to the person taking them - 'therapeutic effects' - while others are undesirable - 'side effects.'
No drug ever developed produces only therapeutic effects with no side effects, because drugs are engineered to interfere with biological processes, and the effects of this interference cannot be precisely controlled.
Here are some of the mechanisms by which PPIs cause their laundry list of adverse effects:
Suppression of gastric acid
The major adverse reactions to PPIs stem directly from the drugs’ therapeutic effect: acid suppression. As mentioned in Part 1, the normal pH of a human stomach ranges from 1.5-3.5 - that is, it is extremely acidic.
This acidity wipes out most bacteria that enter via our nose and mouth, and also prepares iron, calcium and vitamin B12 for absorption in the small intestine.
No wonder then, that the use of PPIs, which reduce stomach acid secretion by up to 99 per cent, leads to small intestinal bacterial overgrowth (SIBO), which in turn may cause up to 80 per cent of cases of IBS.
SIBO further exacerbates nutritional deficiencies caused by acid suppression, in two ways:
The overgrown bacteria compete with us for vitamin B12, reducing the amount available for us to absorb.
The presence of excessive and dysbiotic bacteria in the small intestine triggers chronic release of an iron-regulating hormone called hepcidin, which causes anaemia by reducing the amount of iron available to red blood cells.
Disruption of gut microbiota
Whether or not they develop SIBO, PPI users have fewer commensal (beneficial) gut bacteria in their large intestine, and lower microbial diversity - a key indicator of the health of the gut microbiome.
Specifically, PPI use induces overgrowth of Streptococcaceae and Enterococcaceae, which are risk factors for Clostridioides difficile infection, and decreases growth of Faecalibacterium, an anti-inflammatory microorganism which is known to be an important commensal bacteria.
The implications of PPI-induced imbalances in intestinal bacterial flora are largely ignored by the medical community, but researchers with an interest in the gut microbiome point out that gut dysbiosis is involved in many diseases, including inflammatory bowel disease, diabetes mellitus, obesity, non-alcoholic fatty liver disease, and autoimmune diseases.
Small and large intestinal dysbiosis (imbalanced gut bacteria) are also linked with a higher risk of cardiovascular disease and depression.
Parathyroid effects
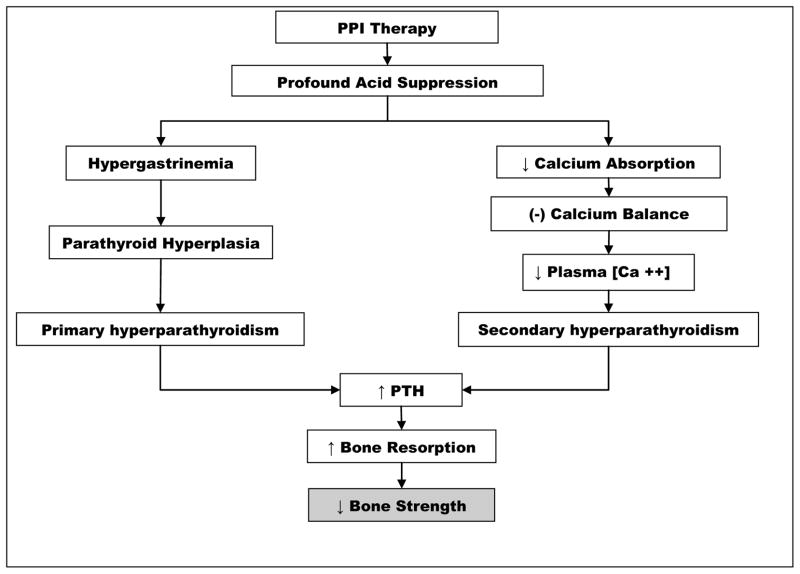
PPIs induce increased levels of the stomach hormone gastrin, which bumps up parathyroid hormone. The reduced calcium absorption caused by acid suppression also increases parathyroid hormone secretion. Higher circulating parathyroid hormone (PTH, in the diagram below) in turn increases breakdown of bone (bone resorption), leading to weaker, more fracture-prone bones:
Thus, PPIs are a double-whammy to bone health, reducing our ability to absorb dietary calcium, and increasing loss of calcium and other minerals from bone.
Endothelial damage
The endothelium is the single layer of cells that form the inner lining of our blood vessels and lymphatic vessels. A healthy endothelium is critical to normal regulation of blood pressure and prevention of atherosclerosis (a build-up of cholesterol-laden plaque inside our arteries); hence, damage to the endothelium leads to vascular diseases including high blood pressure, diabetes, heart disease, heart attack and stroke.
PPIs have been found to impair the function of endothelial cells and accelerate their senescence (the process by which cells become non-functional without actually dying) by reducing their telomere length. This devastating effect on endothelial cells probably explains the increased risk of cardiovascular and kidney disease seen in PPI users, and may even contribute to PPI-associated depression.
Chromogranin A
PPIs increase secretion of a protein called chromogranin A by the adrenal glands; higher levels of this protein have been linked to high blood pressure, heart failure and chronic kidney disease.
This is no doubt just the tip of the iceberg; I'm sure that other mechanisms by which proton pump inhibitors cause both short- and long-term harms will be discovered in the next few years.
The take-home message is that all drugs - even those considered by medical authorities to be safe, such as PPIs which are now even available over the counter in Australia and many other countries - can't 'work' (that is, exert their desired effect) without also exerting undesirable and harmful effects.
PPIs are one of the best-selling classes of drugs of all time, and yet it's only after decades of use that the full extent of their harmful effects, and the mechanisms which cause these harms, are coming to light.
In Part 3, I'll cover how to stop taking PPIs safely, and how you might go about repairing any damage they might have caused.
I am sure the drug companies love all of these side effects because then they can give the victim more drugs to treat the side effects of the PPIs, which then cause more side effects, which leads to even more drugs given. Money, money, money, and more money.
When I was in high school, I learnt that acid plus carbonate reacts to form salt plus water plus carbon dioxide.
Thus HCl + NaCO3 = H2O + CO2 + NaCl.
I always use this for indigestion. 1 teaspoon of BiCarb soda in water, one does only.
The reaction give temporay relief, and allows my stomach to go back to normal acid production.
No nasty co effects, no weird chems in my body, and dirt cheap too.
The only issue the gas, you gotta get that burping right.
I have seen many, many people suffer under PPI meds for days on end with their digestive issues, and yet they refuse to try BiCarb cos their Doctors advise against it. They live in pain for hours/days while a safe and effective treatment is in their Pantry.