


The COVID myocarditis hustle
Health authorities have repeatedly stated that you're more at risk of developing myocarditis from COVID-19 than from the 'vaccine'. They lied.

Remember when the COVID-19 ‘vaccines’ were sold to you as completely safe and effective? Sure you do.
(Wow. That didn’t age well.)
Remember when the authorities who told you they were completely safe and effective, admitted that they ‘very rarely’ cause myocarditis and pericarditis (collectively called ‘myopericarditis’)? You almost certainly do.
Remember when those authorities told you that you should take them anyway, and give them to your kids, because the risk of developing myopericarditis (or other cardiac pathologies) as a complication of COVID-19 was greater than the risk of developing it as an adverse reaction to the experimental transfection agent? And remember when they told you that this very very rare myopericarditis was very very mild? I’ll bet you do.
Remember when a cohort study of 23.1 million residents across four Nordic countries found that the risk of developing myocarditis in the 28 days after two injections of the Pfizer transfection agent was 5.31 times higher in males 16 to 24 years of age than it was in the pre-‘vaccination’ period, during which SARS-CoV-2 was widely circulating? In 16-24 year old males who received two shots of the Moderna product, the risk was 13.83 times higher than in the pre-‘vaccination’ period. Oh, you don’t remember this study being loudly trumpeted by the corporate media? Funny, that. It couldn’t possibly have anything to do with the fact that this study clearly showed that the risk of injection-induced myocarditis in young men far exceeded their risk of infection-induced myocarditis, could it?
Remember when researchers found that the incidence of myopericarditis was 162.2 per million after dose two in US males aged 12–15 (that’s a risk of 1 case of myopericarditis per 6200 boys who received two doses), and 93 per million in males aged 16–17 (risk of 1 in 10,800), compared to a background rate of 2.1/million cases per week in boys); that 86.9 per cent of patients were hospitalised (does that sound ‘mild’ to you?); and that the risk of being hospitalised for myopericarditis after two shots of mRNA transfection agent was 2.8 times higher than the risk of being hospitalised for/with COVID in boys aged 12–15, and 1.6 times higher in boys aged 16–17? You mightn’t remember this one, because the pro-injection ‘experts’ tried to bury it, insisting that it was inappropriate to use the Vaccine Adverse Events Reporting System (VAERS), which was set up by the US government to detect safety signals from vaccines, to conduct research on a safety signal of a vaccine. Because Science™.1
Remember when Swedish researchers published a report on the autopsy findings on 37 people who had died at the Karolinska University Hospital of acute respiratory distress syndrome attributed to COVID-19, and found no replicating SARS-CoV-2 in the heart tissue of the deceased people, and no indications of myocarditis?
“Furthermore, any sign of virus-induced cytopathic effects or any antiviral lymphocytic reaction typical for viral myocarditis was not detected in any cases. Also, signs of antiviral inflammation were not observed. Some studies claim there is a sign of lymphocyte infiltration in the Covid-19 heart [24]. For example, multifocal lymphocytic myocarditis was observed in a small fraction of the cases in a multicenter COVID-19 pathological study [25]. Furthermore, quantitative analysis of inflammatory infiltrates in COVID-19 hearts showed a higher number of CD68+ cells proposing that COVID-19 may cause a different type of myocarditis than conventional viral myocarditis, one that is associated with diffusely infiltrative monocyte/macrophage cells [26]. However, we didn’t detect any lymphocyte or granulocytic infiltration in the Covid-19 cohort as a hallmark of myocarditis.”
Morphological changes without histological myocarditis in hearts of COVID-19 deceased patients
No? You don’t remember that one? I guess it didn’t quite fit the narrative that COVID-19 myocarditis was much more dangerous than injection-induced myocarditis, did it?
Remember when an international team of researchers published a review of all the reports that they could find of people who died of/with COVID-19 in the pre-injection era (a total of 548 deceased people), whose autopsy reports identified cardiovascular pathologies, and found a “low prevalence of myocarditis in COVID-19”?
“The median reported prevalence of extensive myocarditis, multifocal active myocarditis, and focal active myocarditis were all 0.0%, and the median prevalence of inflammatory infiltrate without myocyte damage was 0.6%.”
If you don’t remember it, that’s probably because it received next to no publicity. I wonder why.
Remember the study of 301 Thai teenagers who had ECG, echocardiography, and cardiac enzyme testing performed before and after they received their second shot of Pfizer transfection agent? Almost 30 per cent of these kids had some form of cardiovascular manifestation after the injection, including chest pain, abnormal heart rhythm, high or low blood pressure, and myopericarditis:
“Our study found one case of myopericarditis, four cases of subclinical myocarditis, and two cases of pericarditis among 301 participants.”
Cardiovascular Manifestation of the BNT162b2 mRNA COVID-19 Vaccine in Adolescents
You might remember this one because it did get a bit of airplay, but the part that the presstitutes emphasised was not the fact that seven out of 301 adolescents developed some degree of myopericarditis; it was the authors’ downplaying of their own unbelievably concerning findings, which they waved off with the dismissive comment that the plethora of cardiovascular symptoms that they observed were “mild and transient.”
For starters, no one has any idea what the long-term consequences of injection-induced myocarditis might be; even mild myocarditis with quick recovery is known to significantly increase the risk of heart failure and premature death. And for seconds, even if one were to accept the authors’ description of the cardiac manifestations as “mild and transient”, in what universe is it acceptable to inject an experimental agent that inflicts this degree of suffering on healthy teenagers, for the sake of trying to prevent them from catching a bug that would cause them, at most, a couple of days of flu-like illness?
Finally, do you remember when Israeli researchers published a cohort study of almost 200 000 people, comparing rates of myopericarditis for which hospitalisation was required (i.e. moderate to severe cases), in the pre-injection era, in people who had had COVID-19 (defined as at least one positive PCR test for SARS-CoV-2; yes, I know this is a nonsensical diagnostic criterion but it’s the one the Branch Covidians use, so I’m happy to see them hoist with their own petard), to rates in those who had not… and finding that there was no increase in rates of either myocarditis or pericarditis in people who had had COVID? The rate of myocarditis in post-COVID-19 patients was 0.0046 per cent, while in the control group who had never had COVID-19 it was… 0.0046 per cent. 0.0056 per cent of post-COVID-19 patients were diagnosed with pericarditis, compared to 0.0088 per cent of controls.
What? You haven’t heard of this study? Your doctor didn’t tell you about it, even though it was published in April of last year?
Well, if you weren’t told about any of these studies before being injected with a novel RNA transfection agent, you weren’t given informed consent. If you were told that your teenage son’s risk of getting myocarditis was higher if he got COVID than if got the shot, neither of you was given informed consent (in fact, you were outright lied to). As the Australian Medical Professionals Society (AMPS) has pointed out in a letter sent to all Australian doctors on 11 January 2023, the federal government, the Australian Health Practitioner Regulation Agency and the Australian Immunisation Handbook all oblige Australian doctors and other vaccination providers to obtain informed consent before administering any treatment, including vaccines (or products deceptively labelled as vaccines).
“For consent to be legally valid…It must be given voluntarily in the absence of undue pressure, coercion or manipulation…It can only be given after the potential risks and benefits of the relevant vaccine, the risks of not having it, and any alternative options have been explained to the person.”
Furthermore, AMPS notified doctors that they do not have any government liability protection with respect to the novel COVID-19 transfection agents. And do you know what that means? If you, or a loved one, developed myopericarditis (or any other adverse event that your doctor should reasonably have known about) after receiving a COVID-19 injection, and you were not informed of the risk of this event prior to being injected, you can sue the person who administered the product to you.
Can you imagine how quickly this entire disastrous enterprise could be stopped, if every single person who suffered an adverse reaction, and every single person who lost a loved one, sued the ‘vaccine’ provider for failing to give them informed consent? Professional indemnity insurance premiums would shoot through the roof, doctors and other vaccine providers would refuse to administer the shots for fear of being sued… and who knows, doctors might even remember that their role is to care for their individual patients, not to serve as the commissars of the biosecurity state.
P.S. If you are part of, or know of, a legal firm willing to represent people injured by the experimental injections, please provide contact details in the comments section below.
Legal firms who may be able to assist you with filing suit against a vaccine provider who did not give you informed consent:
https://www.advocateme.com.au/
https://aflsolicitors.com.au/about
http://woodburnsolicitors.com/home.html
https://www.sydneycriminallawyers.com.au/
For information on my private practice, please visit Empower Total Health. I am a Certified Lifestyle Medicine Practitioner, with an ND, GDCouns, BHSc(Hons) and Fellowship of the Australasian Society of Lifestyle Medicine.
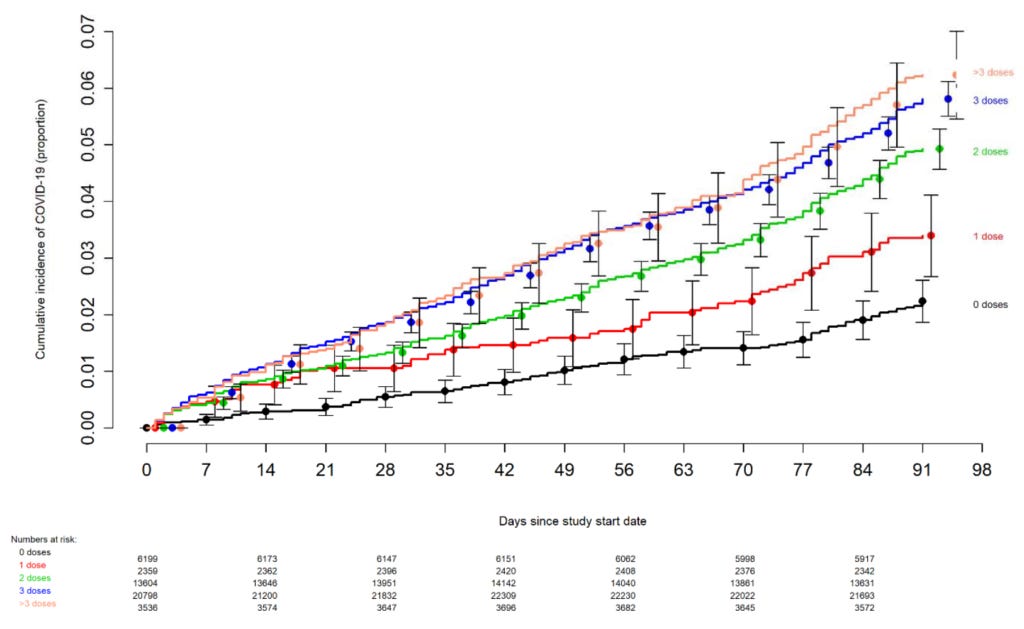
* It's worth pointing out that now that we know that the experimental transfection agent increases your risk of contracting a SARS-CoV-2 infection - remember the Cleveland Clinic study that produced the chart below? - it's a moot point whether COVID or the injection poses a bigger risk of developing myopericarditis.
I do remember those studies because by then I had realised just how much we have to be our own journalists. Sadly, I also think we need to be our own legal system:(https://arkmedic.substack.com/p/die-unfair-arbeitskommission)
Let the lawsuits begin 🔥🔥🔥