


Long COVID: Truth, lies and propaganda - Part 2
Long COVID is not the boogieman we've been threatened with.

In Part 1 of this miniseries, I summarised three studies that suggest that adolescents are not at risk of neurocognitive or psychological symptoms of ‘long COVID’; and that the major risk factors for developing ‘long COVID’ are being physically unwell (including being overweight) and experiencing psychological distress before contracting SARS-CoV-2 infection.
Let's continue exploring the medical literature on long COVID. First up, a study comparing outcomes of COVID and non-COVID respiratory illness:
Study #4: Association of Initial SARS-CoV-2 Test Positivity With Patient-Reported Well-being 3 Months After a Symptomatic Illness
Top-line summary: People who had a non-COVID respiratory illness were more likely to still be unwell three months later, than people who had COVID-19.
The long version:
This US study was a planned interim analysis of an ongoing multicentre prospective longitudinal registry study (the Innovative Support for Patients With SARS-CoV-2 Infections Registry [INSPIRE]) - seriously, who comes up with this stuff? - which was set up specifically to assess long-term outcomes of adults with COVID-19, and to compare them to contemporary controls comprising adults who had similar symptoms but tested negative for SARS-CoV-2 on either a PCR or antigen test.
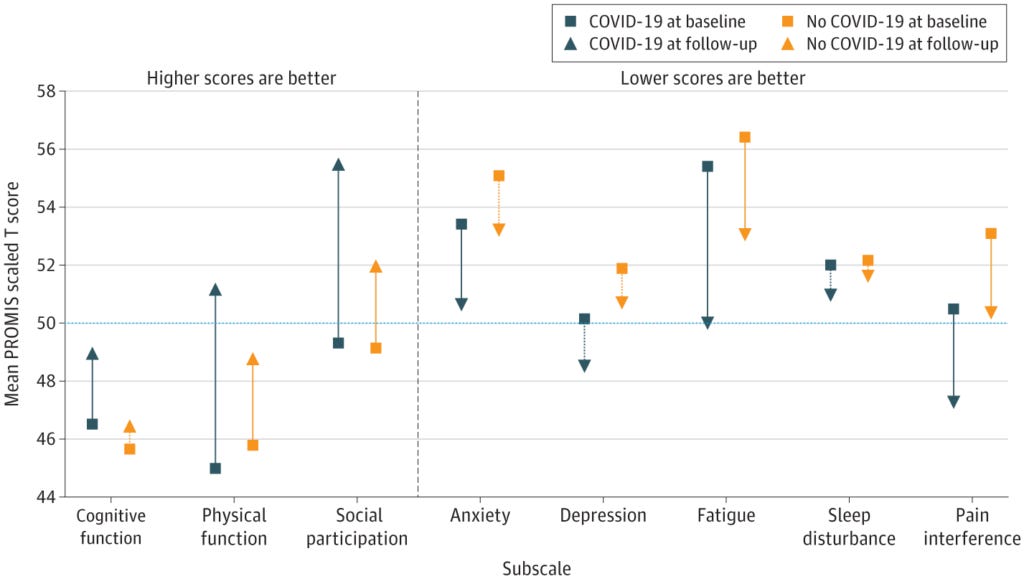
The subjects of this study were the first 1000 participants who completed baseline and 3-month follow-up surveys which used the Patient-Reported Outcomes Measurement Information System (PROMIS-29) - again with the dinky acronyms - to assess their physical function, anxiety, depression, fatigue, social participation, sleep disturbance, and pain interference, and the PROMIS Short Form–Cognitive Function 8a scale to assess cognitive function.
Just over 72 per cent of participants tested positive to SARS-CoV-2 (for what that's worth) while 28 per cent tested negative. (Remember, all participants presented for medical attention with similar symptoms.) Although the rate of moderate to severe impairments across any PROMIS domain were quite similar at baseline (64.7 per cent in the COVID-19–positive group vs 67.4% in the COVID-19–negative group, hinting at just how sick the average American is), the two groups were quite heterogeneous; those who tested negative tended to be older, of non-white race, unmarried, poorer, unemployed, and publicly rather than privately insured, to have been tested for SARS-CoV-2 in an emergency department, and to have moderate or severe asthma, hypertension or diabetes. In other words, those who were not diagnosed with COVID-19 were in worse shape overall at the beginning of the study. Unsurprisingly then, at baseline they were more anxious, depressed, and reported more pain than the COVID-positive group.
Nonetheless, those who tested positive for SARS-CoV-2 reported more symptoms at baseline and were more likely to have been hospitalised for their symptomatic illness. In fact, 10.8 per cent of those who tested positive were hospitalised vs only 1.5 per cent of those who tested negative.
Three months later, almost 40 per cent of people with test-confirmed COVID-19 reported moderate to severe impairments across any PROMIS domain... but so did 53.5 per cent of COVID-19-negative patients. 22 per cent of participants with test-confirmed COVID-19 were moderately to severely anxious or depressed, compared to 27 per cent of participants with a non-COVID illness.
The following chart illustrates the health trajectory of both groups; the 50th percentile line indicates population norms for each metric:
The authors of the study point out the obvious weakness in many other studies that have reported high rates of postviral symptoms - no control group - and also underline the difficulty of distinguishing between genuine postviral symptoms, the effects of delayed or inadequate medical care, and the societal upheaval inflicted by 'public health' policies:
"Although other studies21-24 have found that those who recover from acute SARS-CoV-2 infection are at increased risk of an array of mental health disorders during the subsequent year, participants in the current cohort experienced similar rates of depressive symptoms at baseline and follow-up regardless of initial COVID-19 status. The presence and persistence of poor mental health among nearly 1 in 4 participants (21.9% of the COVID-19–positive group and 27.3% of the COVID-19–negative group) may reflect a more general pandemic exposure, which participants in both groups experienced. The inclusion of a control group of participants who were exposed to the pandemic yet tested negative and the use of validated scores with prepandemic population norms were important to identifying broader pandemic impacts which may have had consequences for observed changes in well-being. For instance, similarity in observed changes in both groups may be reflective of the experience of being ill during a pandemic when access to care was hampered by pandemic restrictions, potentially slowing recovery regardless of the cause of the underlying infection. These broader pandemic societal impacts therefore call for increased attention to mental health services irrespective of SARS-CoV-2 infection status."
Implications of this study:
Poor physical and mental health are shockingly common in the US, and other industrialised nations. People who were already in bad shape before getting acutely ill with a respiratory illness may continue to suffer poor health afterwards, but if anything, those who had a non-COVID illness may do even worse. The brouhaha about long COVID obscures the damage done to people's well-being by non-evidence-based pandemic policies.
Next, a study on postviral symptoms after a mild case of COVID-19:
Study #5: Long covid outcomes at one year after mild SARS-CoV-2 infection: nationwide cohort study
Topline summary: People who experience mild symptoms of COVID-19 have a heightened risk of a small number of conditions, most of which are resolved within a year from diagnosis.
The long version:
This study analysed electronic health records from Maccabi Healthcare Services (MHS), the second largest health maintenance organisation in Israel, which covers a quarter of the Israeli population. The database includes longitudinal data for all COVID-19 diagnoses (counted as a positive PCR test, an extremely problematic diagnostic criterion) and their aftermath, along with detailed demographic information, diagnoses of other conditions, medication prescriptions and pathology test results. The study subjects were all those who were PCR tested for SARS-CoV-2 at least once (comprising 76 per cent of MHS’ members, or over 1.9 million Israelis) but not admitted to hospital with COVID-19 during the 30 days after infection. Patients who tested positive were matched with test-negative patients by age, sex and vaccination status.
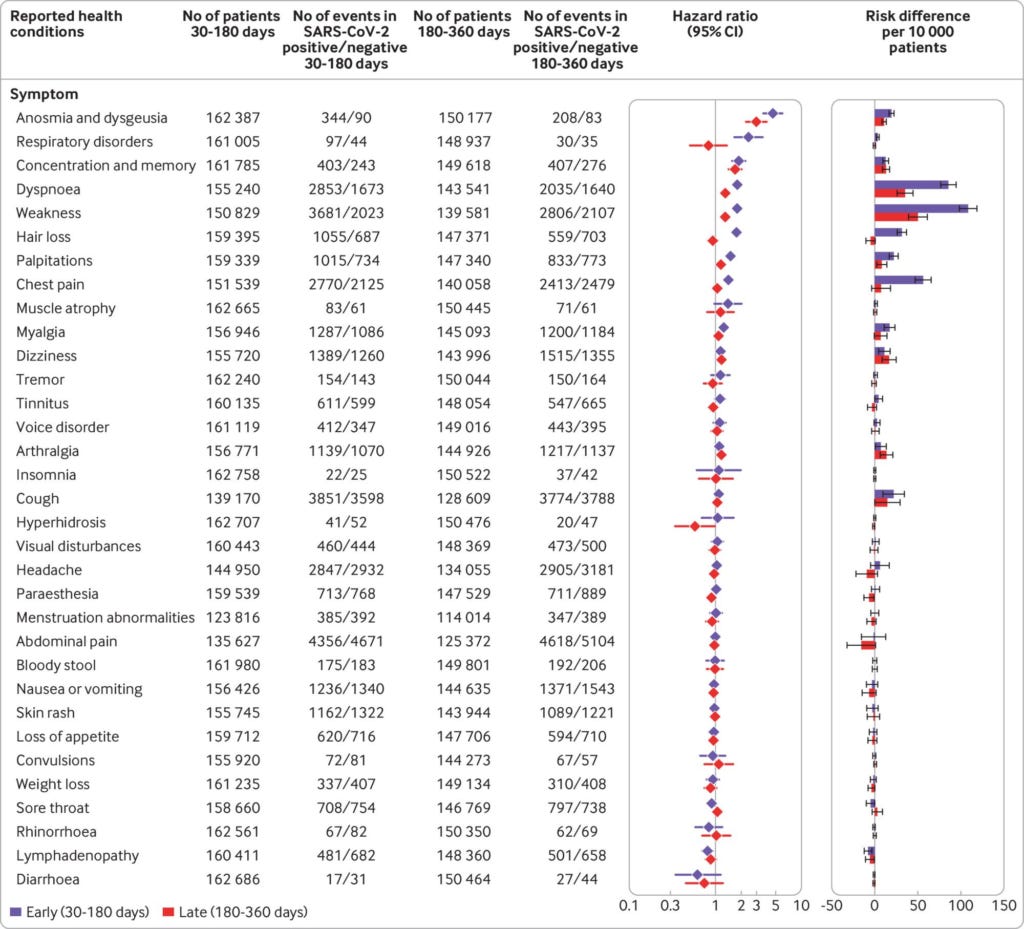
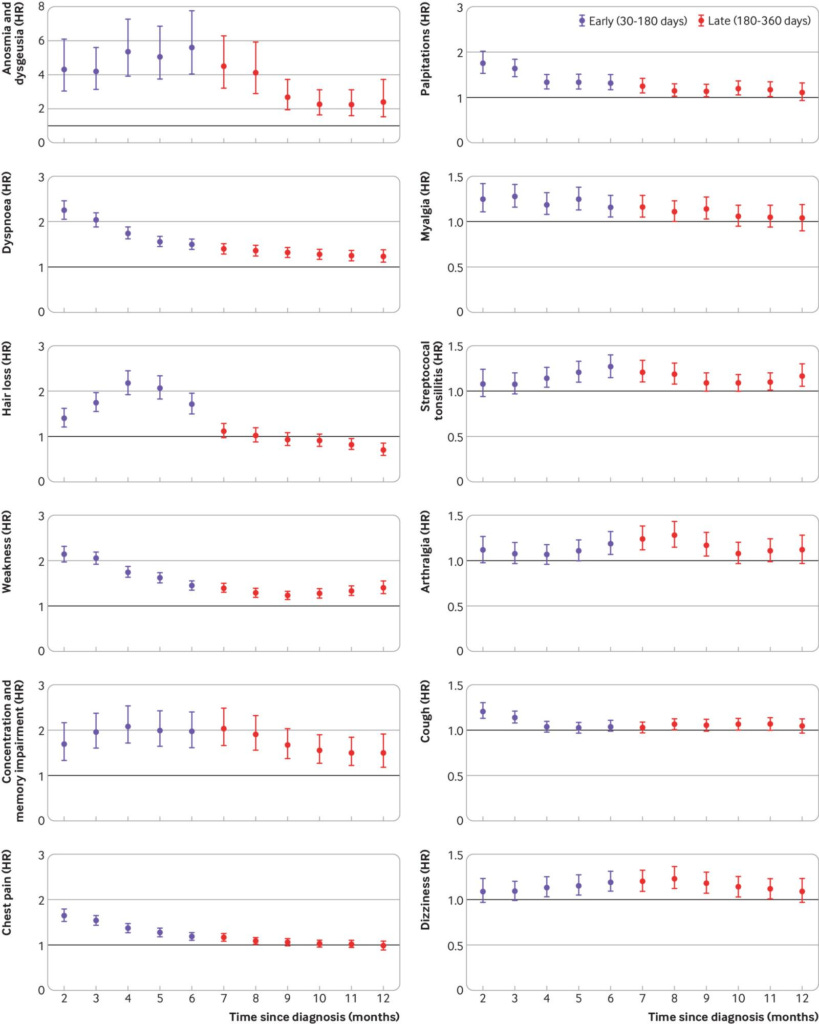
Of all the health outcomes studied, only abnormalities in smell and taste (anosmia and dysgeusia), concentration and memory impairment, breathing difficulties (dyspnoea), weakness, palpitations, streptococcal tonsillitis, and dizziness were significantly more common in people who tested positive for SARS-CoV-2 infection (dots to the right of the vertical line in Figure 2 below), and almost all had completely resolved within 12 months of infection (Figure 3):
The authors stressed that persistent breathing difficulties are common after any respiratory illness, and are no more likely to occur after COVID than after non-COVID disease:
"Dyspnoea emerged as the most frequently reported respiratory symptom in patients with mild covid-19, lasting a year from diagnosis and resulting in increased numbers of prescriptions for related drugs. Nevertheless, the risk of receiving a prescription for a pulmonary diagnosis was independent of SARS-CoV-2 infection, indicating that the pulmonary outcomes following mild covid-19 are not severe and do not need increased drug treatment."
Long covid outcomes at one year after mild SARS-CoV-2 infection: nationwide cohort study
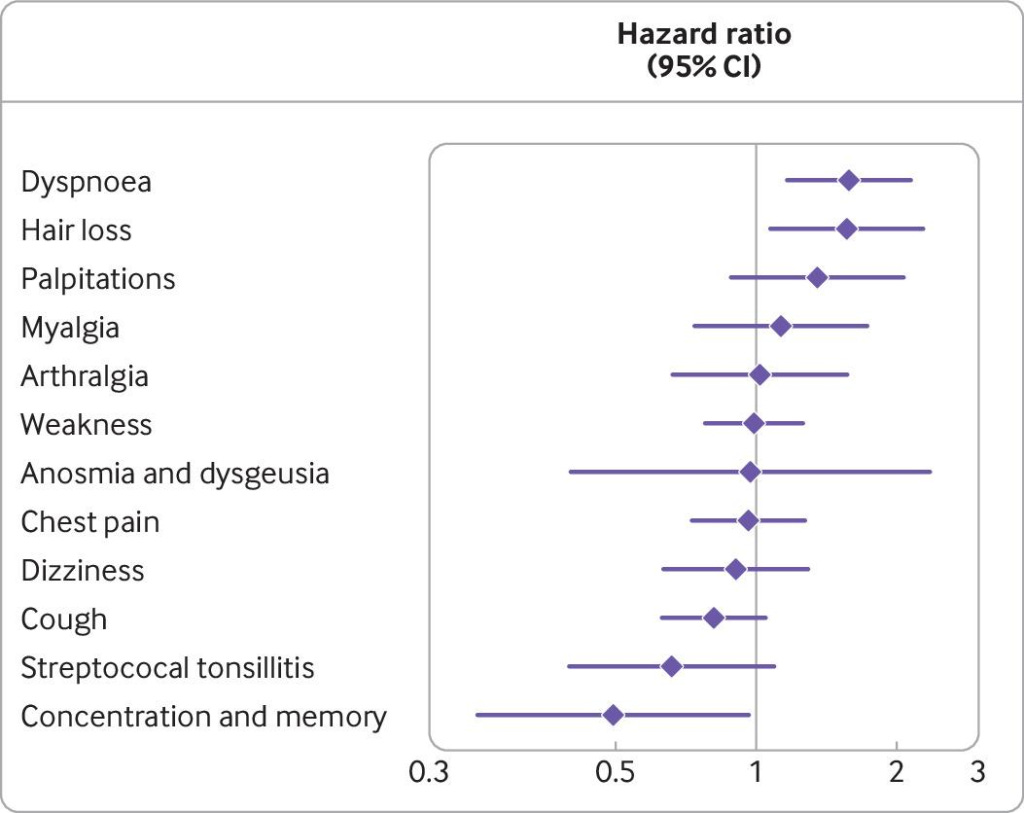
The study also compared health outcomes in people who tested positive to SARS-CoV-2 after getting an mRNA transfection agent ("COVID vaccine") vs those who were not injected. Only people who tested positive at least 14 days after their second injection were counted as "vaccinated". Research indicates that people have a higher risk of becoming infected in the two weeks after their first shot, yet anyone whose positive test result occurred in this time period was lumped into the 'unvaccinated' category. Notwithstanding this diagnostic sleight-of-hand, only breathing difficulties and hair loss were reported significantly more commonly in unvaccinated COVID patients, while impaired concentration and memory occurred significantly more commonly in the vaccinated.
Implications of this study:
The risk of 'long COVID' was one of the sticks used to beat people who resisted getting an experimental injection into submission. People who knew they were at negligible risk of suffering a severe case of COVID-19 were told that they should still get vaccinated to reduce the chances of developing long COVID. But people who have a mild case of COVID have about the same risk of suffering prolonged postviral symptoms as they would after any other viral respiratory disease, and vaccination makes little to no difference in that risk.

Next, let's look at whether COVID 'vaccines' prevent long COVID:
Study #6: The effectiveness of coronavirus disease 2019 (COVID-19) vaccine in the prevention of post–COVID-19 conditions: A systematic literature review and meta-analysis
Topline summary: COVID 'vaccines' reduce the absolute risk of developing long COVID by a clinically insignificant 1.5 per cent.
The long version:
This 'study of studies' analysed data from ten studies on the efficacy of COVID vaccines in reducing long COVID symptoms. The definitions of 'long COVID' used in each of these studies were all over the map, ranging from symptoms lasting more than three weeks to symptoms continuing for over six months post-infection. One study did not report the duration of symptoms defined as 'long COVID' at all.
Four of the studies evaluated vaccine effectiveness in preventing 'long COVID' among those who received the COVID-19 vaccine only after having COVID-19, three studies evaluated vaccine effectiveness for post–COVID-19 conditions among those who were vaccinated before having COVID-19, two looked at vaccine effectiveness among those who were vaccinated both before and after COVID-19, and one did not specify the timing of the vaccine in relation to having COVID-19.
Five studies found no benefit of COVID-19 vaccination in reducing post–COVID-19 condition symptoms while four showed a protective effect, and one did not report any statistical analysis of effectiveness.
The meta-analysis of the six studies which evaluated post–COVID-19 conditions among those who received at least one dose of a COVID-19 vaccine before or after having COVID-19 found that
"The pooled prevalence of post–COVID-19 conditions was 39.1% among those who were unvaccinated and 37.6% among those who received at least 1 dose."
That's a 1.5 per cent reduction in absolute risk, for the mathematically challenged. Wow, that's impressive.
All the studies included in the review and meta-analysis were observational rather than randomised, which the authors admit introduces multiple biases (including the 'healthy user bias', which Mathew Crawford has written about extensively, and which probably accounts for the entirety of observed vaccine efficacy).
Furthermore, the authors were not able to perform any analyses about possible adverse events after vaccination as only one of the included studies reported possible vaccine adverse events.
Implications of this study:
People who were sold on the idea of taking a COVID jab to prevent long COVID have been sold a bill of goods. With a 1 in 800 risk of suffering a serious adverse reaction to a COVID 'vaccine', any benefit of these injections in preventing long COVID (which is most likely an artefact of the healthy user bias in any case) pales into insignificance.
And finally, what protects people against developing long COVID?
Study #7: Adherence to Healthy Lifestyle Prior to Infection and Risk of Post–COVID-19 Condition
Topline summary: People who follow healthy lifestyle practices have a reduced risk of long COVID, and the more healthy lifestyle practices, the lower the risk.
The long version:
This study enrolled participants in the long-running Nurses’ Health Study II cohort. Participants were assessed for their adherence to six healthy lifestyle habits:
Healthy body mass index (BMI of 18.5-24.9);
Never smoking;
At least 150 minutes per week of moderate to vigorous physical activity;
Moderate alcohol intake (5 to 15 g/d);
High diet quality (upper 40 per cent of Alternate Healthy Eating Index–2010 score); and
Adequate sleep (7 to 9 h/d).
Among those who had tested positive to SARS-CoV-2 with either an antibody, antigen, or PCR test, there was a stepwise decrease in the risk of post-COVID conditions, defined as symptoms lasting for longer than four weeks after a bout of COVID, with increasing number of healthy lifestyle factors:
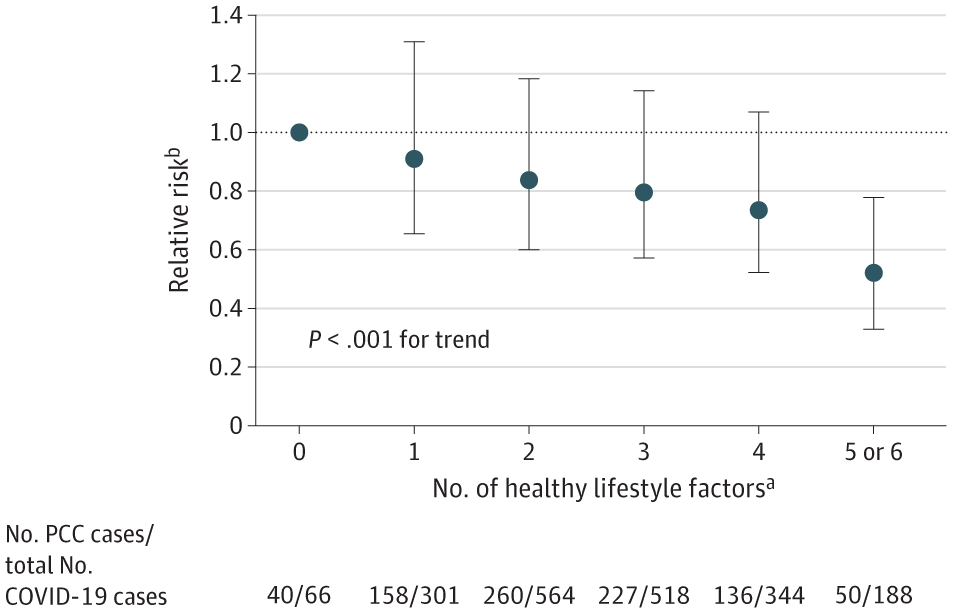
The authors calculated the relative risk of developing long COVID in participants with the most vs the fewest healthy lifestyle factors, and also the population attributable risk percentage (PAR). PAR is an estimate of the proportion of long COVID in this cohort that hypothetically would not have occurred if there was truly a causal relationship between healthy lifestyle factors and long COVID, and all participants were in the low-risk group:
"Compared with women who did not adhere to any healthy lifestyle factors, those having 5 or 6 factors had a 49% lower risk of PCC [post-COVID conditions]... Assuming a causal relationship, the PAR for healthy lifestyle was 36.0% (95% CI, 14.1%-52.7%)."
Adherence to Healthy Lifestyle Prior to Infection and Risk of Post–COVID-19 Condition
In plain English, 36 per cent of long COVID symptoms would not have occurred if all participants had adhered to five or six healthy lifestyle factors.
Being overweight and getting inadequate sleep turned out to be the strongest risk factors; the PAR overweight/obesity was 10.3 per cent (i.e. roughly one in ten participants who had postviral symptoms would not have had them if they were a healthy weight) while the PAR for inadequate sleep was 6.6 per cent.
The authors propose three biological mechanisms linking unhealthy lifestyle factors with an increased risk of long COVID:
Chronic inflammation: Each of the six unhealthy lifestyle factors that they examined has previously been shown to be associated with chronic inflammation, while sustained systemic inflammation has been implicated in the development of post-COVID conditions.
Dysregulation of adaptive autoimmunity: Unhealthy lifestyle factors derange immune function, and dysregulated adaptive autoimmunity has been found in individuals with long COVID.
Blood clotting abnormalities: These are seen in people with obesity, smoking, physical inactivity, and excessive alcohol intake, and pathophysiological changes in blood clotting have been observed in people with long COVID.
Implications of this study:
In Part 1 of this miniseries, we saw that fat, sick people were more likely to develop long COVID. This study provides evidence of the corollary: people who take care of their health are less likely to suffer from postviral symptoms, and the more healthy lifestyle behaviours an individual practises, the lower their risk.
Summing up
The 'long COVID' bugaboo is just one thunderclap in what Professor Mark Crispin Miller has labelled an "ever-rolling thunder of Big Lies". Postviral syndromes do occur, and they definitely do cause distressing and life-limiting symptoms in a minority of people. However, 'long COVID' is no more common nor severe than postviral syndromes after other infections; it's not prevented by COVID 'vaccines'; and the strongest protective factors are the healthy lifestyle behaviours that reduce the risk of every other chronic condition.
If governments had invested our taxpayers' dollars into making sure that everyone had access to healthy, fresh food instead of issuing stay-at-home orders that drove up reliance on home-delivered food; encouraged exercise rather than closing gyms, parks, beaches and playgrounds; and issued calm, accurate messages about risk rather than ginning up fear and anxiety which drove many people to booze, smoke and binge on junk food and Netflix, we would not only have avoided a large percentage of long COVID cases; we would have had a healthier population overall.
But then, those would be the actions of a government that actually served the interests of its people rather than its corporate masters, wouldn't it?
I was once in a lengthy email debate with a 'Christian' organisation about COVID vaccines. They were hyper-pro-vax and could not fathom a world without Pfizer their lord and saviour. Anyway, after refuting all of their tripe for several months the leader of this group eventually wished "long COVID" on me for defying their admonitions to take a shot for Science. It's the closest Ive ever come to having long COVID, or COVID, this entire 3 years. Sigh.