


Long COVID: Truth, lies and propaganda - Part 1
What is 'long COVID', who's really at risk of developing it, and why?

Back in November 2021, I wrote an article called The “long COVID” PSYOP, about the weaponisation of the syndrome of persistent postviral symptoms after SARS-CoV-2 infection, aka 'postacute sequelae of SARS-CoV-2' (PASC), aka 'long-haul COVID', aka 'long COVID'. In that article, I stressed that postviral syndromes do genuinely occur after a wide variety of viral infections, but that the threat of 'long COVID' had been blown out of all proportion to its actual prevalence and severity. I also contended that one of the principle motivations for doing so was to terrorise people into accepting an experimental vaccine which they were (falsely) promised would protect them against this bogeyman.
Since then, numerous articles have been published on long COVID which only confirm my thesis from 16 months ago.
Over the next few posts, I'm going to walk you through some of these studies. Let's get started with a study that set out to discover whether teenagers are at risk of detrimental psychological and cognitive outcomes of COVID-19:
Study #1: Comparison of mental health outcomes in seropositive and seronegative adolescents during the COVID19 pandemic
Top-line summary: There was no difference in the prevalence of neurocognitive, general pain and mood symptoms in adolescents who had been infected with SARS-CoV-2 vs those who had not.
The long version:
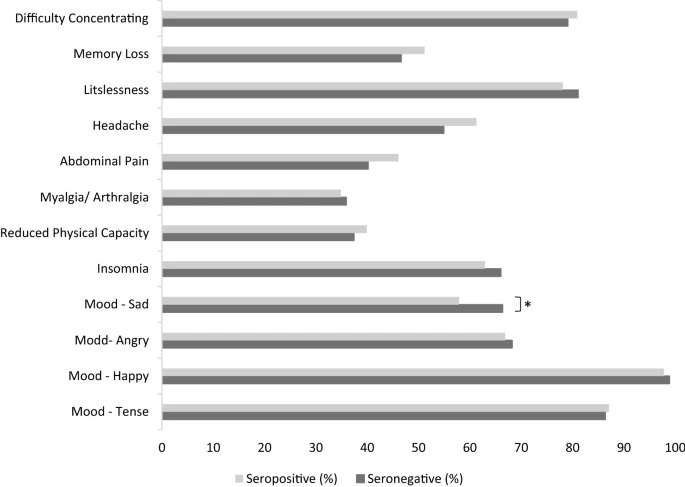
In this study, 1560 German high school students underwent regular blood tests for antibodies to SARS-CoV-2, indicating that they had been exposed to the virus (with or without developing symptoms of infection). The adolescents also responded to a 12 question long COVID survey which asked them if they had experienced any of the following symptoms in the previous seven days: difficulty concentrating, memory loss, listlessness, headache, abdominal pain, muscle or joint pain, reduced physical capacity, insomnia, or changes in mood (happy/sad/angry/tense).
Rather worryingly, each of these symptoms was reported by at least one-third of the students in the previous seven days... but there was no statistically significant difference between reporting rates in kids who had been exposed to SARS-CoV-2 vs those who hadn't, with one strange and inexplicable exception: those who had been infected were significantly less likely to report having experienced sad mood (indicated by the asterisk in the figure below). Go figure.
Female students reported a consistently higher prevalence of neurocognitive, pain and mood symptoms compared to male students, in keeping with a large body of research showing that a mental health 'gender gap' opens up in adolescence and persists through adulthood, with females having significantly higher prevalence of common mental health disorders than males (particularly in countries with the greatest commitment to gender equality, paradoxically enough).
There was no difference in the prevalence of long COVID symptoms in adolescents who already knew they had had a SARS-CoV-2 infection vs those who were found to have antibodies to the virus but didn't report being diagnosed with infection.
The authors pointed out that previous studies that had found a high prevalence of symptoms attributed to long COVID in children and adolescents, had no uninfected control group. Furthermore, they suggested that their results indicated that many, if not most, of these symptoms were likely caused or exacerbated by the impact of public health policies such as school closures and (anti)social distancing on the well-being of young people.
Implications of this study:
The threat of a tsunami of long COVID in children and adolescents has not materialised. Ill-considered, poorly-targeted, non-evidence-based pandemic policies have had a far more negative impact on young people's well-being than COVID-19 itself.
Study #2: Associations of Depression, Anxiety, Worry, Perceived Stress, and Loneliness Prior to Infection With Risk of Post–COVID-19 Conditions
Top-line summary: People who were already experiencing psychological distress before experiencing a SARS-CoV-2 infection are more likely to report symptoms of 'long COVID'.
The long version:
This study recruited nearly 55 000 participants, who were already enrolled in one of three large, long-running and predominantly female cohort studies: the Nurses’ Health Study II, Nurses’ Health Study 3, and the Growing Up Today Study. The average age of participants was 57.5 years, and nearly two in five (38 per cent) were employed in health care.
Participants were eligible to participate if they had no evidence of SARS-CoV-2 infection in April 2020. They answered a questionnaire to assess their levels of depression, anxiety, worry about COVID-19, perceived stress, and loneliness at baseline, and were then followed up with periodic surveys on their psychological function, COVID-19-related symptoms, degree of life impairment and any positive SARS-CoV-2 test results, until November 2021.
Fascinatingly, during 19 months of follow-up, while a supposedly highly-contagious respiratory virus was supposedly wreaking havoc on the world, only six per cent of participants reported a positive result on a SARS-CoV-2 antibody, antigen, or polymerase chain reaction test. Remember, 38 per cent of participants were actively employed as health care workers during the study, and presumably many of them were directly involved with the care of patients diagnosed with COVID-19, and most or all would have undergone regular testing. Yet 94 per cent of participants didn't get infected.
Of participants who did report a positive SARS-CoV-2 test result during the follow-up period, 44 per cent reported post–COVID-19 conditions. Of these, 87 per cent said their symptoms lasted two months or longer, and 56 per cent reported at least occasional daily life impairment related to post–COVID-19 conditions.

The most common symptoms were fatigue (56 per cent), smell or taste problems (44.6 per cent), shortness of breath (25.5 per cent), confusion/disorientation/brain fog (24.5 per cent), and memory issues (21.8 per cent).
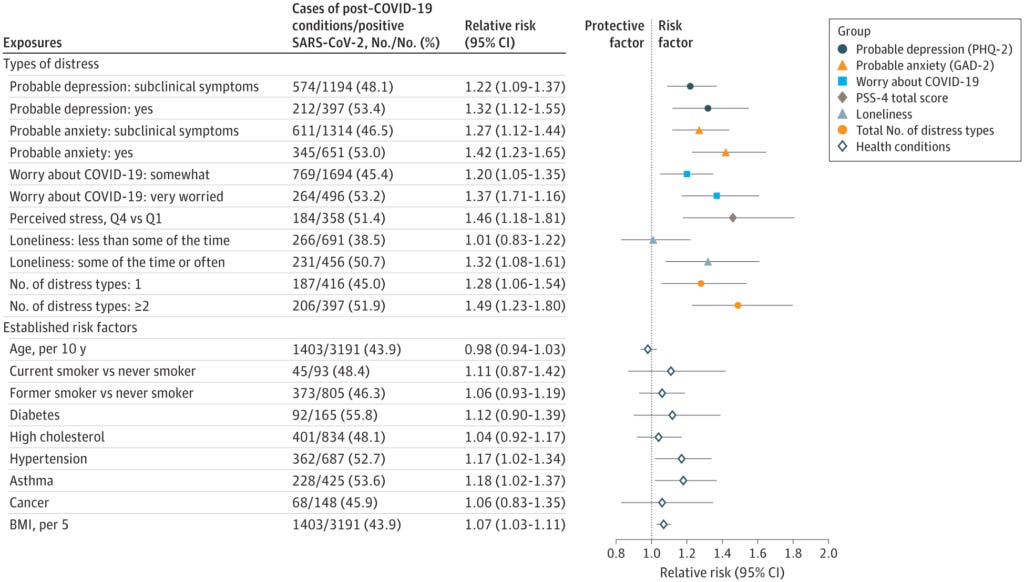
After adjustment for demographic factors, all the types of psychological distress assessed at baseline were significantly associated with an increased risk of post–COVID-19 conditions:
Participants who had probable depression at baseline had a 39 per cent higher risk of long COVID symptoms;
For probable anxiety, the risk was 47 per cent higher;
Those who were very worried about COVID-19 had a 43 per cent higher risk;
Those who perceived their stress level to be the highest had a 50 per cent higher risk than those with the lowest perceived stress;
Those who reported feeling lonely some of the time or often were at 35 per cent higher risk;
Participants with two or more types of distress had a 54 per cent higher risk of reporting long COVID symptoms than those with none.
And here's something really interesting: psychological distress was a stronger predictor of long COVID symptoms than established risk factors for developing severe COVID-19 (which is a known predictor of long COVID risk) including age, obesity and diabetes. In fact, older participants were at lower risk of developing long COVID than younger participants.
Check out this forest plot, which depicts the magnitude of various risk factors for predicting long COVID (the further the coloured symbol is to the right of the vertical line, the higher the risk; symbols to the left of the line indicate reduced risk):
Another interesting finding was that the only long COVID symptoms that tended to be more common in participants who were not psychologically distressed at baseline were the symptoms most characteristic of COVID-19 itself: persistent cough, and problems with taste and smell:
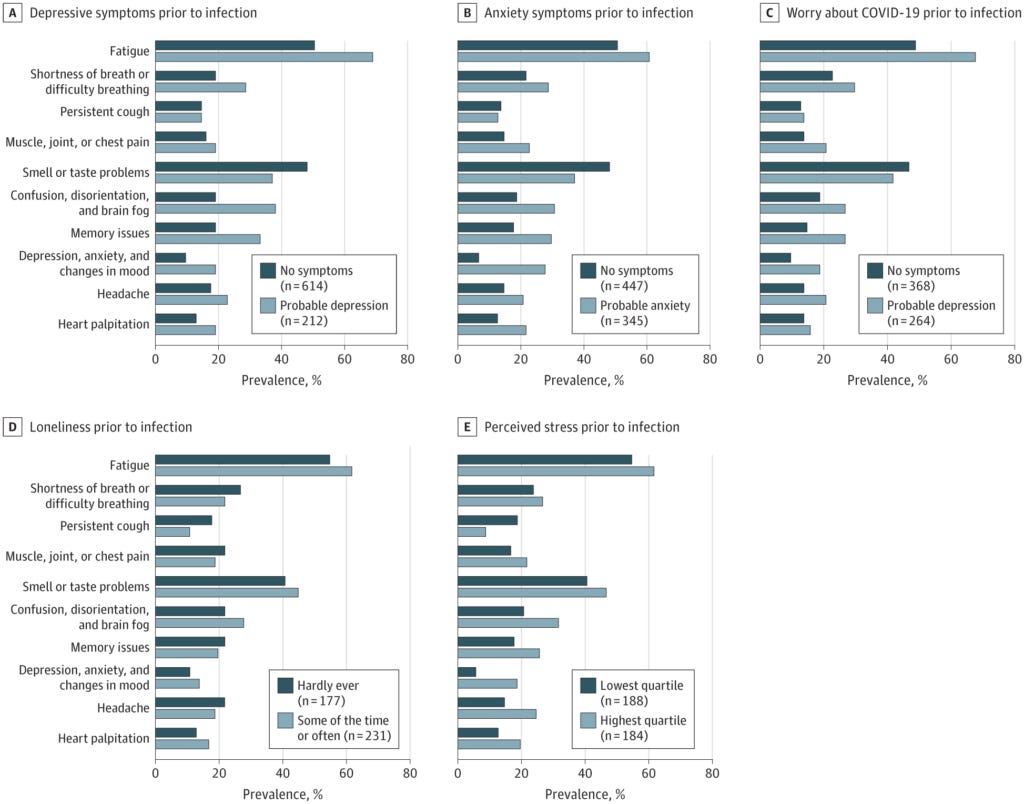
It was the more nonspecific symptoms - such as fatigue, brain fog, mood changes - that were more likely to be reported in participants with pre-infection psychological distress.
So does that mean that the persistent symptoms reported by psychologically distressed people are 'all in their heads'? No, say the researchers. Here's their proposed mechanism that links a perturbed mind to long COVID symptoms:
"Inflammation and immune dysregulation may link psychological distress with post–COVID-19 conditions. Distress is associated with chronic systemic inflammation, resulting in sustained production of proinflammatory cytokines and reactive oxygen species.19-23 Inflammatory cytokines have been proposed as possible causes of respiratory, neurological, cardiovascular, muscular, and gastrointestinal long-term COVID-19 symptoms.51-53 In addition, stress activates the hypothalamic-pituitary-adrenal axis, which can lead to chronic immune suppression. Immunosuppressive conditions have been found to be associated with risk of persistent symptoms after COVID-19,12 but findings were not conclusive.13,54,55 Furthermore, autoantibodies have been associated with both mental health conditions and post–COVID-19 conditions.14,56 In the central nervous system, mental health disorders are associated with chronic low-grade inflammation and microglia activation, which may cause cognitive impairment and long-term fatigue.57 Hypometabolism in the frontal lobe and cerebellum, a pathopsychological change associated with major depression, has also been implicated in post–COVID-19 fatigue.58-60"
In other words, there are measurable disturbances in the physiology of people who are suffering from psychological distress, and these disturbances have profound and multifactorial effects on the ability of these people to fight off infection and recover from its effects.
(I’ve discussed the link between inflammation and impaired psychological and physical functioning in several previous articles, including Inflammation: why you’re fat, sick, tired, depressed and in pain… and what to do about it, Rumination inflammation and Hearts, minds and bodies on fire: Loneliness, social isolation, inflammation and COVID-19.)
Implications of this study:
People presenting with long COVID should be assessed for psychological distress, and the treatment plan must include comprehensive and effective strategies for addressing it.
Study #3: Long-lasting Symptoms After an Acute COVID-19 Infection and Factors Associated With Their Resolution
Top-line summary: The factors most strongly associated with having long COVID are those most strongly associated with having any chronic disease: obesity, older age, and being anxious or depressed.
The long version:
This study involved over 53 000 participants in three French population-based cohorts, who were surveyed about persistent COVID-19 symptoms, defined as "symptoms occurring during the acute infection and lasting 2 or more months".
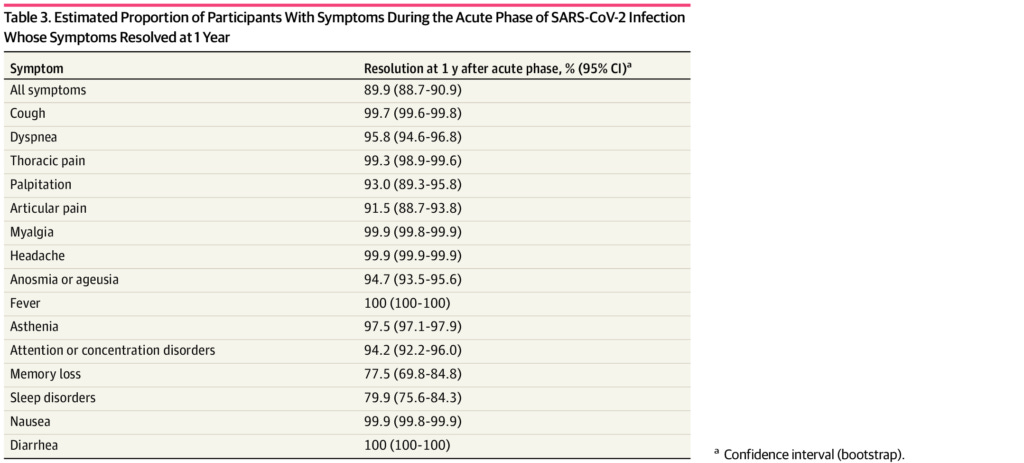
Of those who were infected by SARS-CoV-2 during the first wave of COVID-19 in France (confirmed by antibody testing), fully one third reported no symptoms of COVID-19 whatsoever. Of those who did report acute symptoms, 90 per cent were fully recovered within 12 months, and 92 per cent after 18 months.
The persistent symptoms that were least likely to resolve were memory loss, sleep disorders, joint pain, heart palpitations, loss of taste or smell and attention or concentration disorders:
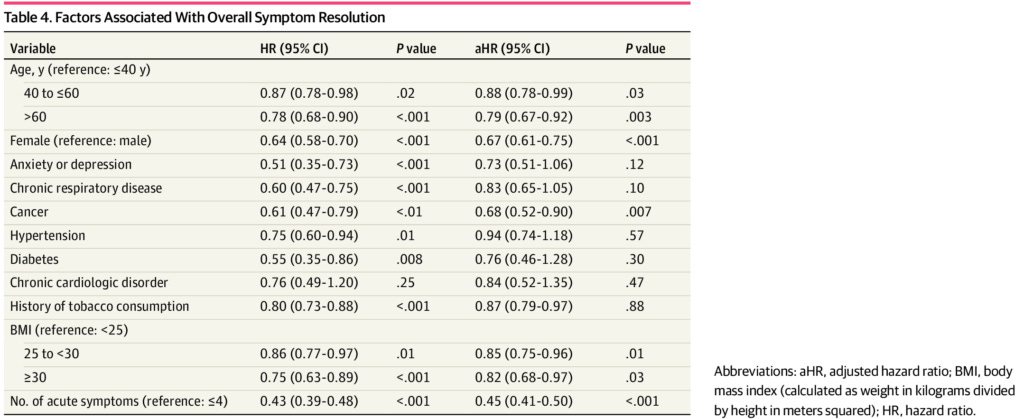
Where things get really interesting though, is the analysis of factors associated with delayed recovery. Those factors were: being older than 40 (and especially older than 60), female, anxious or depressed, obese, suffering from chronic respiratory disease, having five or more symptoms of acute COVID-19, or having a history of cancer, diabetes or cigarette smoking. (After statistical adjustment for unspecified factors, older age, female sex, obesity, history of cancer or smoking, and having five or more acute COVID-19 symptoms remained statistically significant.):
In other words, being already in a state of poor physical and/or mental health made participants less likely to recover from a viral respiratory illness. What a surprise.
Implications of this study:
Fat, sick people are more likely to become seriously ill when they contract a respiratory illness (as I explained in my previous article When Two Pandemics Collide: How obesity affects COVID-19) and more likely to have a delayed or incomplete recovery. That's because they're fat and sick. If our 'health authorities' were genuinely interested in reducing the burden of 'long COVID' they would be pivoting our disease care system to a true health care system focused on preventing chronic illness and treating it with evidence-based lifestyle medicine programs, rather than squandering taxpayers' dollars on an ever-growing arsenal of pharmaceuticals.
Stay tuned for Part 2 of this series!
Happily, the placebo effect remains fascinating, and one of the best uses of studies is to identify it. Sadly, there is no better example of the type of war being waged than this: our brightest minds feel compelled to explain why imaginary conditions are imaginary, and reiterate that being fat and unhealthy is unhealthy.