


How many people have COVID-19 injections harmed?
Part 2

In Part 1 of this article series, I shared data from the Australian, US, European and UK pharmacovigilance systems on the number of reported adverse reactions to COVID-19 injections. I also shared whistleblower testimony from Ahpra-registered healthcare providers, revealing how few of these adverse events are actually being reported in Australia.
The underreporting of adverse events occurring after receipt of a COVID-19 injection is not confined to this country.
Thanks to whistleblowers and data analysts, we’re able to get some sense of just how massive this underreporting is. Let’s take a brief look at some of the many estimates that have been made so far.
1. CMA whistleblower – multiply reported adverse events by at least 5
According to a computer programmer with access to US Medicare and Medicaid data maintained by the Centers for Medicare and Medicaid Services (CMS),
“VAERS (the Vaccine Adverse Event Reporting System) database, while extremely useful, is under-reported by a conservative factor of at least 5. On July 9, 2021, there were 9,048 deaths reported in VAERS. I verified these numbers by collating all of the data from VAERS myself, not relying on a third party to report them. In tandem, I queried data from CMS medical claims with regard to vaccines and patient deaths, and have assessed that the deaths occurring within 3 days of vaccination are higher than those reported in VAERS by a factor of at least 5. This would indicate the true number of vaccine-related deaths was at least 45,000. Put in perspective, the swine flu vaccine was taken off the market which only resulted in 53 deaths.”
2. Jessica Rose’s analysis of VAERS data – multiply reported severe adverse events by at least 31
Polymath Jessica Rose (who has degrees in Applied Mathematics, Medicine in Immunology, Computational Biology, Molecular Biology and Biochemistry) has intensively analysed VAERS data and concluded that severe adverse events are underreported by a factor of at least 31. Shockingly, she calculates that
“Using this URF [underreporting factor] for all VAERS-classified SAEs [severe adverse events], estimates to date are as follows: 205,809 dead, 818,462 hospitalizations, 1,830,891 ER visits, 230,113 life-threatening events, 212,691 disabled and 7,998 birth defects to date.”
You can watch Dr Rose’s stunning testimony to the FDA here and download the slides from her presentation here.
3. Mathew Crawford and Jessica Rose’s joint analysis of data from VAERS and Mass General study – multiply reported severe adverse events by at least 41
Using multiple methods to validate their calculations, Crawford and Rose “computed a 41X under-reporting factor for serious adverse events in VAERS, leading to an estimate of over 150,000 excess deaths caused by the vaccine.”
Their conclusion is stark:
“There is no evidence that these vaccines save more lives than they cost. Pfizer’s own study showed that adverse events consistent with the vaccine were greater than the lives saved by the vaccine to yield a net negative benefit. Without an overall statistically significant all-cause mortality benefit, and evidence of an optional medical intervention that has likely killed over 150,000 Americans so far, vaccination mandates are not justifiable and should be opposed by all members of the medical community.”
4. Ronald Kostoff et al’s analysis of VAERS and CDC data – multiply reported injection-related deaths by at least 100
Kostoff – another polymath – and his highly experienced international team took a deep dive into CDC reported deaths and VAERS data and concluded that “the actual number of deaths strongly related to the COVID-19 inoculation should be scaled up by factors of 100-200”. Furthermore,
“A novel best-case scenario cost-benefit analysis showed very conservatively that there are five times the number of deaths attributable to each inoculation vs those attributable to COVID-19 in the most vulnerable 65+ demographic. The risk of death from COVID-19 decreases drastically as age decreases, and the longer-term effects of the inoculations on lower age groups will increase their risk-benefit ratio, perhaps substantially.”
Please read those two sentences again, just to let their meaning sink in.
In fact, let’s spell it out in very plain English: In people aged 65 and over, the number dying as a consequence of receiving a COVID-19 injection is at least 5 times greater than the number who died of/with COVID-19. And for younger people whose risk of dying of COVID-19 is much lower, the odds of being killed by the shot rather than the illness against which it is meant to be protective are even higher.
Is there real-world confirmation that COVID-19 injections are killing more people than they’re saving?
1. United Kingdom
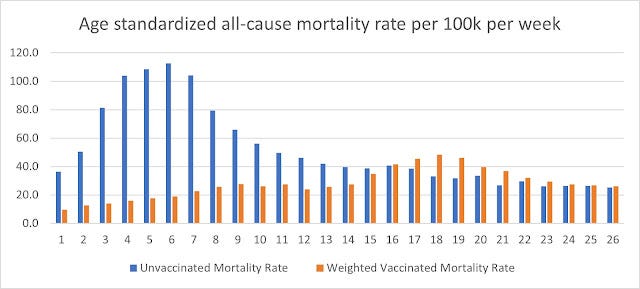
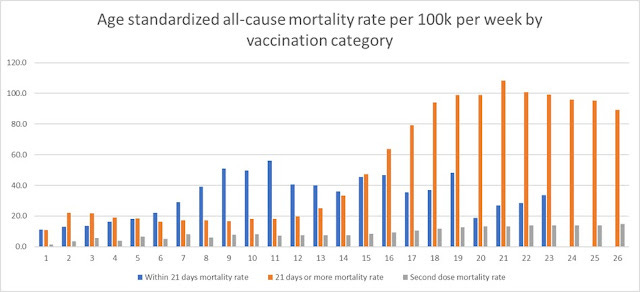
Norman Fenton and Martin Neil’s analysis of all-cause mortality in the UK found that
“The death rate is currently higher among the vaccinated than the unvaccinated.”
And, while mortality rate in the unjabbed conformed to the normal seasonal trend of a winter peak followed by a steady decline throughout summer, exactly the opposite occurred in those who had received COVID-19 jabs: a completely unseasonal rise in summer.
2. Scotland
Having jabbed 91% of people aged 16 and over (with 84% “fully vaccinated”), Scotland’s excess mortality – that is, deaths exceeding those expected for the time of year – was running at 25% above the five-year average in mid-September.
“There has been a sustained period of excess deaths, with registered deaths above the five year average in each week since week 21 (24th to 30th May).”
Not only were deaths attributable to COVID-19 at their highest level since March (the tail-end of the winter mortality bulge which runs from December to March); non-COVID deaths were also up by 10%.
If the jabs work so well, why are more people dying from COVID-19 now in Scotland – and the rest of the UK – than they were at this time last year, with no “vaccine” available? And why are more people dying from other causes?
3. Israel
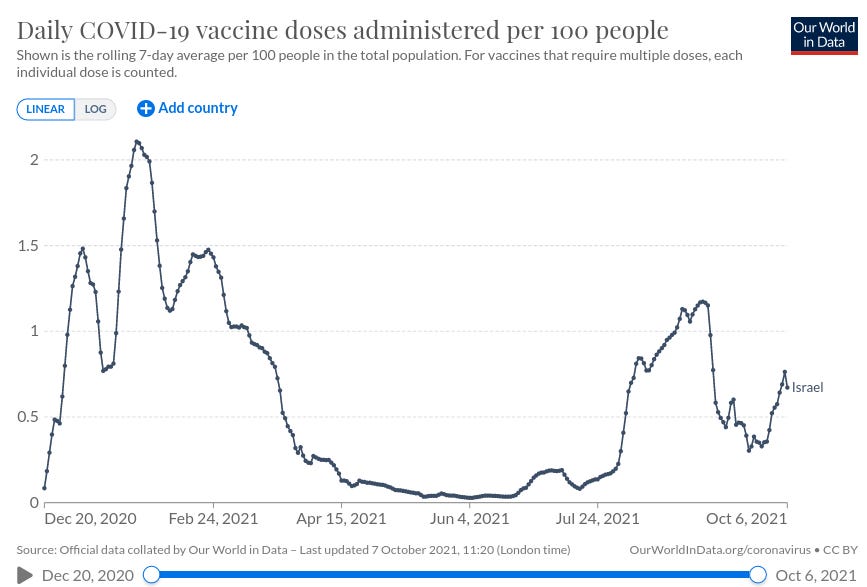
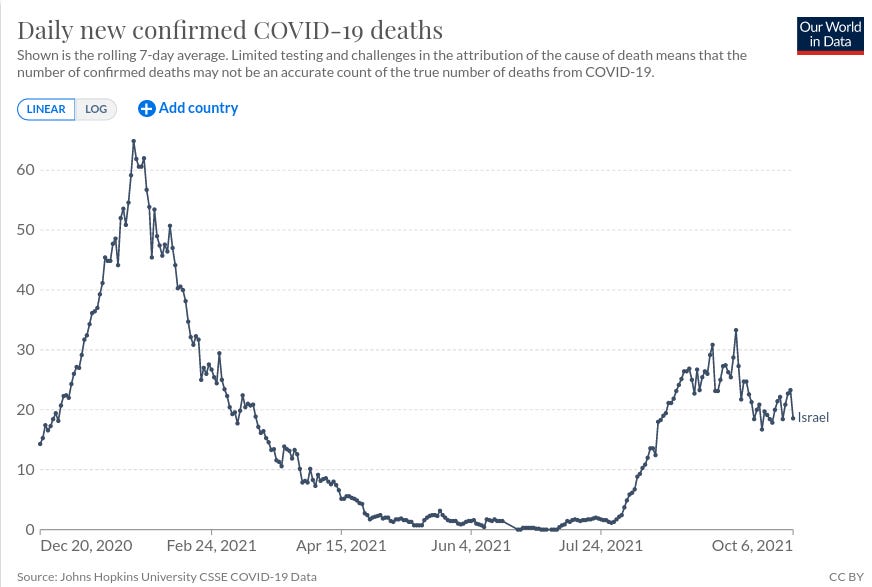
Israel’s government signed a secret contract with Pfizer, trading the confidential medical data of its entire population for priority access to experimental jabs. After rushing those jabs into the arms of almost its entire population over the age of 16, the country enjoyed a lull in cases and deaths. This respite terminated abruptly in mid-summer, prompting the deployment of a third, “booster” injection.
Notice how closely the jab rollout mirrors deaths attributed to COVID-19:
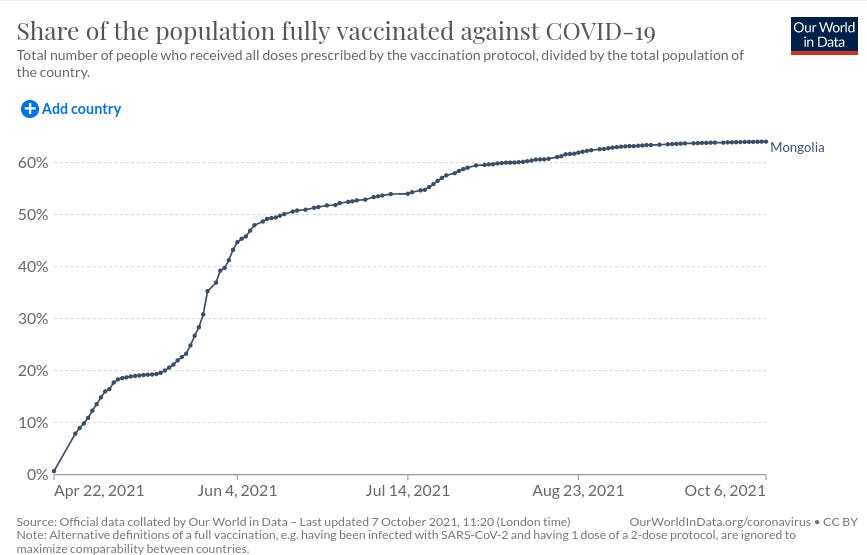
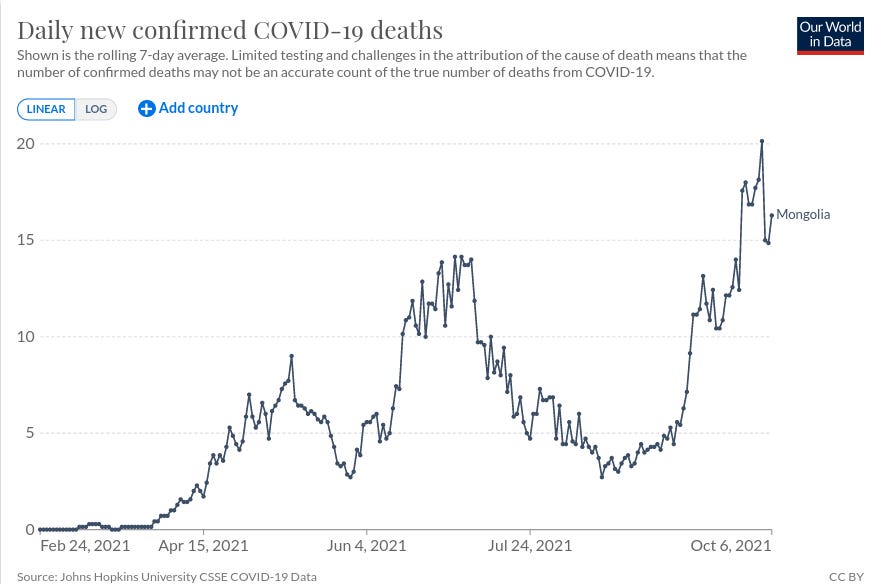
4. Mongolia
Mongolia experienced almost no COVID-19 related deaths until it commenced its “vaccine” rollout. Why, with 67% of its entire population jabbed (64% “fully”), is its daily COVID death toll markedly higher than in the pre-jab era?
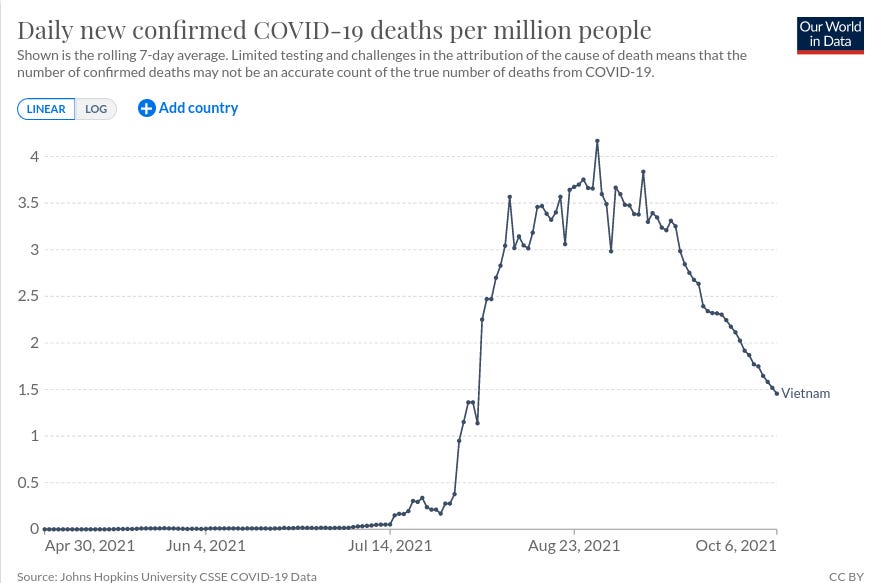
5. Vietnam
This southeast Asian nation was effusively praised for its response to COVID-19, racking up barely 500 cases and no deaths until July 31, 2020, despite sharing a border with China. Its effective early treatment policy (based on hydroxychloroquine) resulted in an impressively low case fatality rate (CFR). However, after abandoning hydroxychloroquine for convalescent plasma in early August 2020, the CFR suddenly shot up:
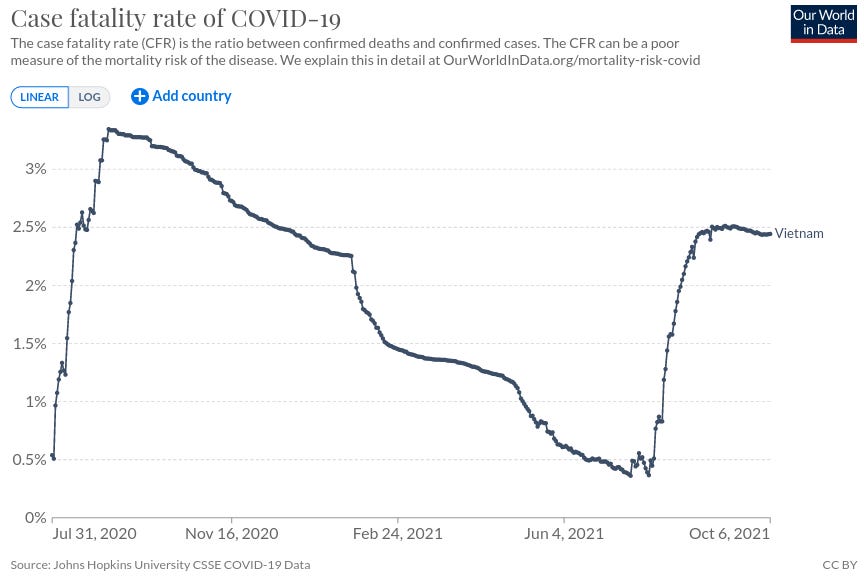
Vietnam’s COVID-19 injection campaign started slowly, but notice how the CFR began to pick up as the rollout gathered steam.
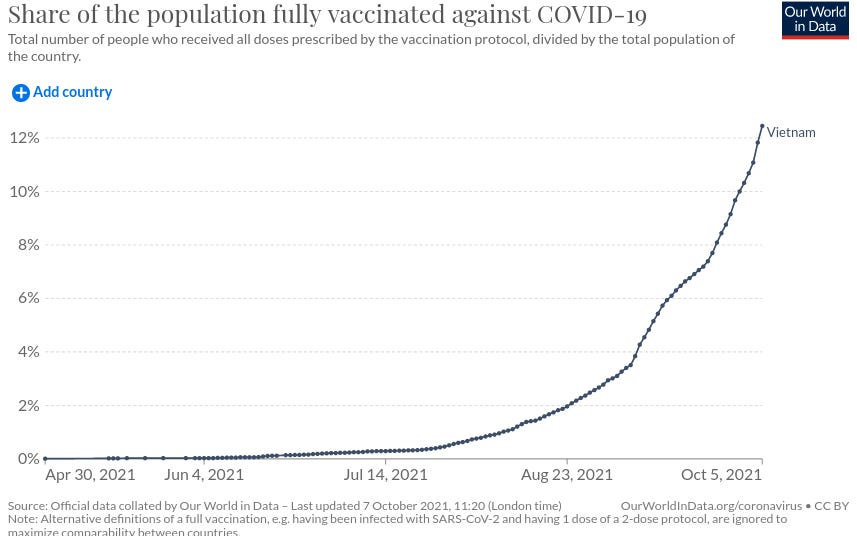
And while its COVID-19 mortality rate remains low by international standards, deaths began to spike after jabs started going into arms – the exact opposite of what we would expect if these products truly reduced deaths from COVID-19.
There are many more examples that I could give, and I encourage you to explore country profiles from Our World in Data for yourself to see what patterns you find.
Suffice it to say that the story we’ve been sold about “life-saving vaccines” is not backed by empirical data. More people are dying of both COVID-19 and non-COVID causes than in the pre-injection era.
Just how many people have been harmed by these inadequately-tested products? No one knows. As described above, it could be as few as five times as many as has been reported to pharmacovigilance systems, right through to more than 200 times as many.
Although the scientists and data analysts cited above differ in their estimates, they all agree on one fact: there is no population group for whom the benefit of taking COVID-19 shots outweighs the risk. And as Kostoff et al stress,
“We have no idea what the death numbers will be in the intermediate and long-term… Since many of these potential serious adverse effects have built-in lag times of at least six months or more, we won’t know what they are until most of the population has been inoculated, and corrective action may be too late.”
If you believe there is a God, now might be a good time to start praying.