


Goldilocks and the iodine bears
Not too little, not too much...

In my February Open Thread for paid Substack subscribers, dentist extraordinaire Dr
, whose Substack is one you really should be subscribing to, asked me to investigate whether hypothyroidism is being overdiagnosed and overtreated. It's a great question, and I will be answering it in my next post.To set up for that post, however, I thought it was worth delving into the role that iodine plays in human nutrition, health and disease. Why is it important to understand what iodine does, and what are the consequences of both under- and overconsumption of this critical micronutrient? Firstly, because thyroid hormones are actually made from iodine, so if you are not consuming enough iodine, you will develop some type of thyroid dysfunction. Secondly, many 'alternative' practitioners are promoting the use of wildly excessive doses of iodine supplementation, which cause more problems than they solve - including thyroid disease.
That leads me to the crucial question, which I'm sure occurred to you when you read the title of this article:
Wtf does Goldilocks have to do with iodine?
When I was growing up, Goldilocks and the Three Bears was simply an entertaining, if morally ambiguous, tale about a little girl with a concerning lack of respect for the property rights of other people (or ursines), rather than an embodiment of racist stereotyping of non-Caucasian ethnicities and an instantiation of white privilege...
https://twitter.com/Laughin_Man/status/878343521220136960
... and systemic racism...
https://twitter.com/PeterWMurphy1/status/1350317030453387264
... not to mention a golden - pardon the pun - opportunity to teach anti-racism to a captive audience of six year olds.
(Every day, I feel grateful that a) I grew up in the 1970s, before all this crap, and b) my children are no longer in the government indoctrination camp known as the public school system.)
But white supremacist overtones aside, the eponymous juvenile delinquent-in-training gifted the English language one of its most evocative phrases: the Goldilocks principle. Across a wide range of disciplines, from developmental psychology to biology, astronomy, economics and engineering, the Goldilocks principle refers to the quantity or range of some important factor that is not too much, not too little, but just the right amount, for the proper operation of a particular system.
The Goldilocks principle, applied to nutrition, means that for every micronutrient and macronutrient, there is an amount or range that is just right for us to thrive. Iodine is no exception to this rule. Too little iodine intake causes both hypothyroidism (underactive thyroid) and hyperthyroidism (overactive thyroid), goitre (swelling of the thyroid gland) and cretinism (now more commonly known as congenital hypothyroidism, a severe physical and mental retardation caused by impaired thyroid hormone production in utero due to inadequate maternal iodine intake). But too much iodine intake also causes both hypo- and hyperthyroidism, goitre and thyroid cancer.
Iodine: Vulcan's gift, delivered by Neptune?
The outer iodine cycle
Iodine occurs in the earth's crust at a concentration of approximately 0.14 mg/kg. All rocks and soil contain some iodine, but those of volcanic origin have much higher concentrations, as volcanoes dredge up elements from deep in the earth's core and spew them out over the surface of our planet. Marine soils, in particular, are rich in iodine which dissolves into seawater (reaching concentrations of 50-60 μg/L, or 0.05-0.06 mg/L) and is taken up by phytoplankton, which convert it into a form that can be absorbed by seaweeds. Seaweeds can accumulate iodine at up to 30,000 times its concentration in seawater. The seaweeds then convert iodine into a form which can be evaporated into water vapour, to be deposited on land in the form of precipitation, which can then return iodine to soil. Furthermore, seaweeds emit iodine in gaseous form, which influences cloud formation in coastal regions. And on top of all this, seaweeds help to remove the strong reactive oxygen species, ozone, from the lower atmosphere. Isn't nature cool?
That gaseous iodine may even contribute to the iodine intake of people who live in coastal regions rich in seaweed beds, by being inhaled. Sea air really is good for you!
Unsurprisingly, foods of marine origin - seaweeds, shellfish and fish - are the major dietary sources of iodine. The iodine content of terrestrial-sourced foods is dependent on local soil levels of iodine, and whether any deficiencies are addressed through soil amendment or supplementation of animal feed. More on that topic shortly.
The inner iodine cycle
The iodine that we consume from food or supplements is converted into the iodide form within our stomach and duodenum (upper small intestine). 90 per cent of ingested iodine is absorbed. It circulates in the bloodstream and is taken up primarily by the thyroid gland, which accumulates it at a concentration 20 to 50 times greater than in blood plasma (rendering a blood test for iodine status completely useless).
Depending on how much iodine is circulating, the thyroid gland will take up as little as less than 10 per cent to more than 80 per cent of it. Iodine released from the catabolism of thyroid hormones can be recaptured out of the bloodstream by the thyroid gland to make more hormones. Any excess iodine is excreted via the urine and in fact, 90 per cent of the iodine we consume ends up being urinated out, assuming adequate iodine intake.
Iodine is an essential trace element - that is, a mineral that is required for the continuation of life, but only in tiny amounts. Its essentiality arises from the fact that it is a constituent of the thyroid hormones, thyroxine (T4) and triiodothyronine (T3) - indicated by the 'I's in the molecular diagrams below. Iodine makes up the majority of the weight of both hormones:
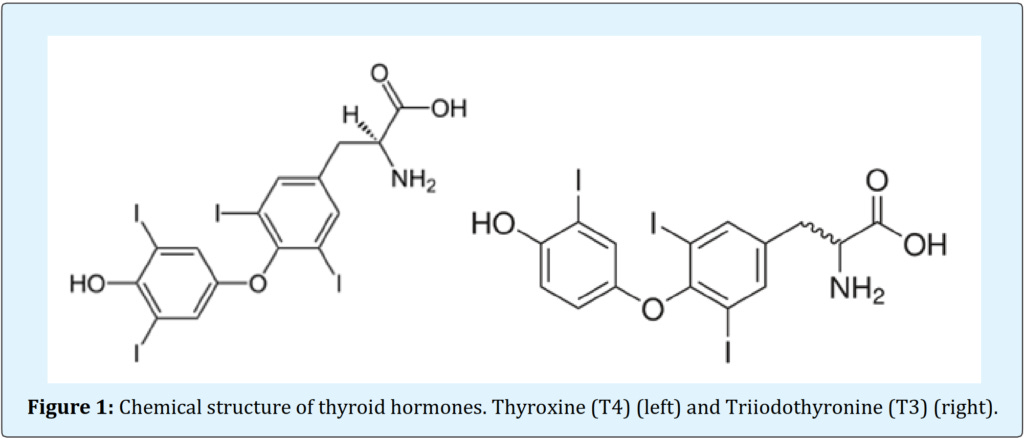
Other organs besides the thyroid gland which take up iodine from the bloodstream include the stomach, breast, and skin. Some researchers have proposed that the low breast cancer rates observed in Japanese women may be partially attributable to their high intake of iodine, primarily via seaweed. This possible benefit must be offset against the higher risk of papillary carcinoma of the thyroid documented in Japanese women who regularly eat seaweed; this form of cancer is, fortunately, usually slow-growing and rarely fatal.
How much iodine do we need?
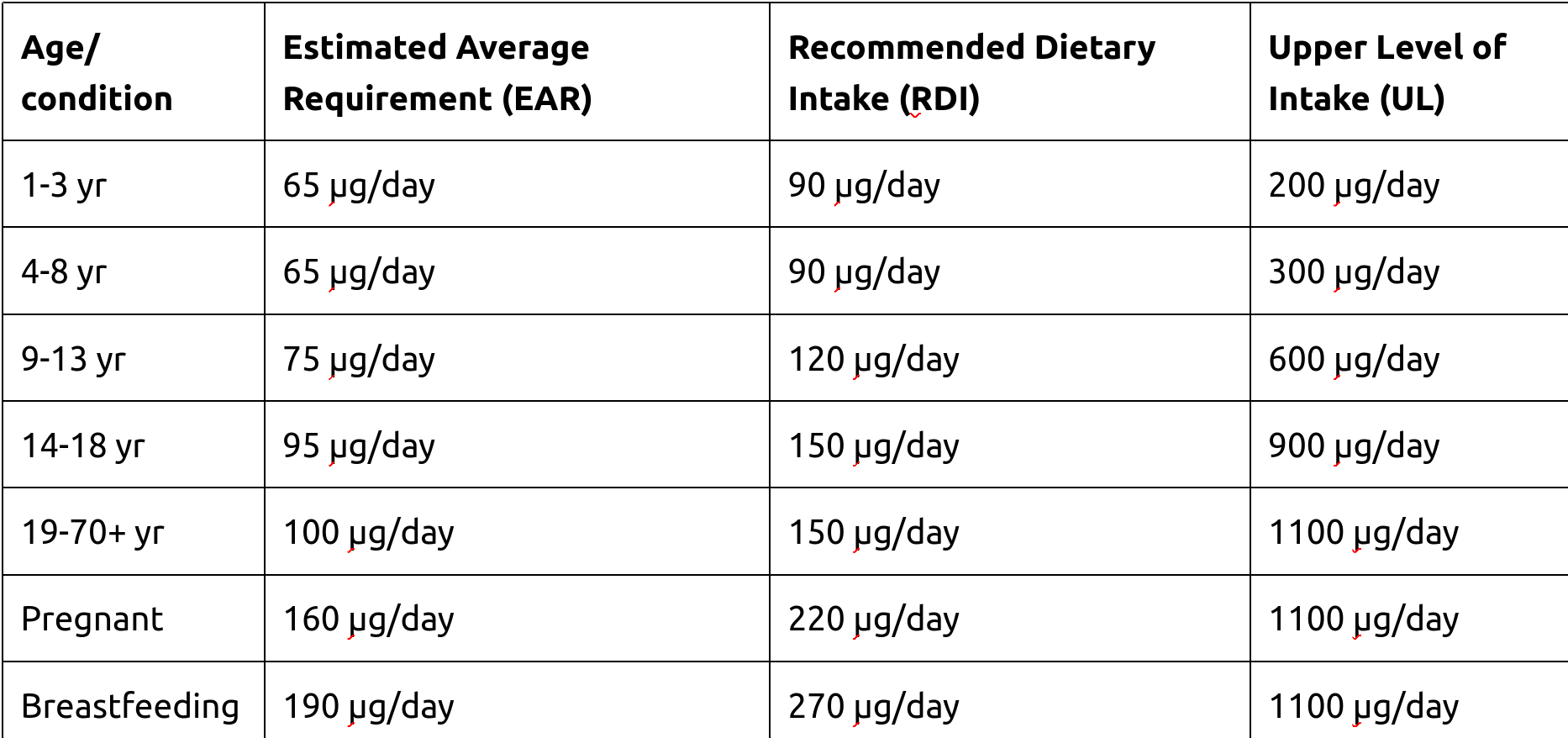
The National Health and Medical Research Council has developed the following recommendations for iodine intake, based primarily on iodine balance studies:

The tragic consequences of iodine deficiency
Endemic iodine deficiency plagues populations that subsist on locally-produced food grown in iodine-depleted soils, with devastating consequences for health, intellectual potential, and both personal and national productivity. Sadly, almost one third of the global population lives in such regions, mostly in remote and mountainous areas of South-East Asia, Latin America and Central Africa - notably, some of the poorest places on Earth.
Even mild iodine deficiency can compromise cognitive development. For example, the Avon Longitudinal Study of Parents and Children (ALSPAC) cohort found that children born to mothers in Britain whose urinary iodine excretion in the first trimester of pregnancy was below recommended levels (indicating inadequate iodine intake), had lower verbal IQ and reading ability at age nine.
Note that Britain has long been considered iodine replete (i.e. most of the population is getting enough iodine), unlike the many poor countries which are acknowledged to have high rates of iodine deficiency. When average daily iodine intake falls below 25 μg, congenital hypothyroidism begins to appear - and with it, growth stunting and lifelong reduction in mental potential. Children exposed to severe iodine deficiency during growth lose an average of 12.45 IQ points. In fact, dietary iodine deficiency is the leading cause of preventable cognitive impairment in the world.
In the light of this, it's shocking that two billion people on Earth consume an inadequate amount of iodine. That's a tremendous loss of human potential that could be corrected unbelievably cheaply, through food fortification programs, and/or mass distribution of iodine supplements to women of childbearing age, which would prevent congenital hypothyroidism and the lifelong constraints on development that it inflicts.
The salt iodisation program introduced in the US in the 1920s dramatically improved iodine nutriture in the population, reducing the prevalence of goitre from 5 per cent of World War 1 recruits to 0.06 per cent of World War 2 recruits. Likewise, the mandatory iodine fortification of salt used in commercial breadmaking, implemented by Tasmania in 2001, and Australia and New Zealand in 2009, led to improvements in population iodine status (with significant differences in iodine adequacy between those who did, and did not, eat bread daily).
But how would the 'structural racism' crowd signal their virtue if one of the major contributing factors to economic inequality both within and between nations - nutritionally-induced IQ reduction of a significant proportion of the population - was actually resolved, at fairly minimal cost and without a single struggle session? And how would philanthrocapitalists continue to turn a profit out of "giving" to impoverished countries, if they ploughed money into iodine supplementation rather than - just as a for instance - vaccination programs?

In addition to cognitive impairment, dietary iodine deficiency can cause hypothyroidism (due to inadequate production of thyroid hormones), thyroid nodules and goitre. Surprisingly, hypothyroidism is less common in iodine-deficient than in iodine-replete regions, while hyperthyroidism shows the opposite pattern, an anomaly that I'll discuss further in the next post. Correction of long-term iodine deficiency in later life can, unfortunately, lead to thyrotoxicosis ("thyroid storm"), underlining the importance of preventing deficiency in pregnant women and children.

The dangers of excess iodine
There are many case reports, and a few clinical studies, documenting the effects of excessive iodine intake, most commonly from seaweeds, kelp supplements, iodine supplements, iodine-containing drugs, and topical iodine-based antiseptics.
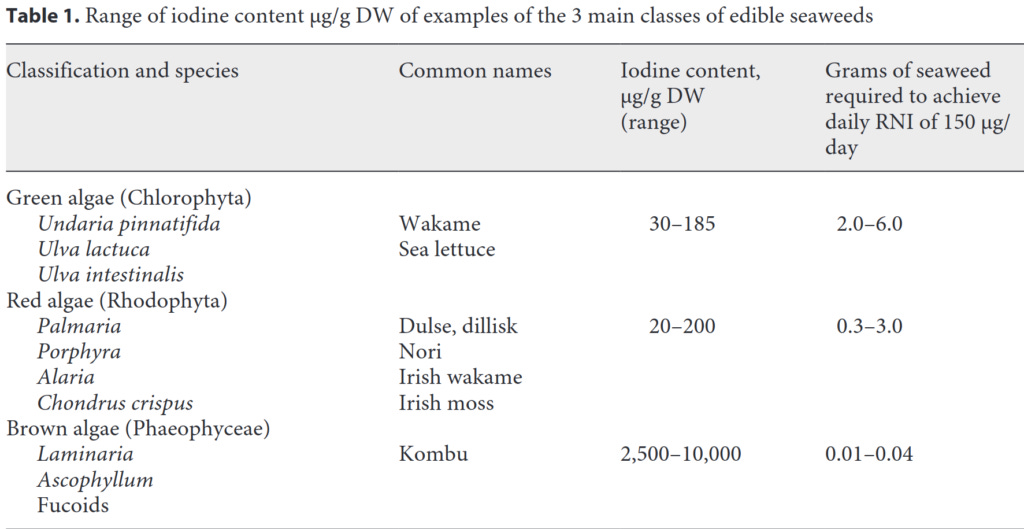
The iodine content of seaweeds is quite variable, depending on a number of factors including the species, stage of growth, size of the plant, season, and geographical location. Brown seaweeds (kelps, also known as kombu) generally containing more iodine than the green or red varieties. Some varieties of kelp can contain up to 8 mg of iodine per gram.
Below is an indication of possible iodine intake arising from consumption of the major types of seaweeds, drawn from a number of different publications. Notice how consuming even 1 gram of kelp/kombu would result in exceeding the upper tolerable daily iodine limit of 1100 μg per day set for adults:
In a study conducted in Japanese adults, both short- and long-term consumption of 15 g per day of kombu (containing 35 mg - that's milligrams, not micrograms - of iodine) caused a sustained elevation of TSH, the pituitary hormone that regulates thyroid hormone production. Circulating levels of thyroid hormone were slightly decreased by short-term kombu consumption, but barely affected by long-term intake. This picture - elevated TSH with normal T4 and T3 - is known as subclinical hypothyroidism, and I'll be discussing it at length in the next post.
Likewise, Lugol's solution, which is recommended by many 'alternative' practitioners, is a strong solution of potassium iodide that contains 50 mg - again, that's milligrams, not micrograms - of iodine per mL. Because it's so concentrated, the correct dosage is measured in drops, and accidental overdoses are common, occasionally leading to death. In any case, Lugol's is not intended for use as an iodine supplement, but to shrink the size of the thyroid gland, to suppress thyroid hormone release during thyrotoxic crisis and after thyroid surgery, and to block uptake of radioactive iodine in a radiation exposure emergency.
Excessive iodine intake can, rather confusingly, cause both hypo- and hyperthyroidism. In fact, as mentioned above, hypothyroidism is actually more common in areas with excessive iodine intake than with normal iodine intake. And just like inadequate iodine intake, it can cause goitre; the term “endemic coastal goitre” was coined in 1965 to describe iodide-induced goitre in the residents of Hokkaido, Japan.
Perhaps most disturbingly, given the propensity of some practitioners to recommend high dose iodine supplementation to everyone with a diagnosed or suspected thyroid condition, overloading on iodine can induce thyroid autoimmunity (Hashimoto's thyroiditis or Graves' disease), which accounts for the majority of thyroid conditions diagnosed in countries that are iodine-replete.
Remember how Goldilocks rejected both the too-cold and the too-hot porridge? As mentioned above, both too little and too much iodine are hazardous to health. So how do we know whether we're taking in just the right amount?
Assessing iodine status: It's complicated
The health-o-sphere is increasingly dominated by people obsessed with measuring and quantifying everything, from daily steps, to time spent in stage 3 sleep, to minute-by-minute fluctuations in blood glucose level. It's as if Sesame Street's Count von Count grew up to be a biohacker. Perhaps as a result of this zeitgeist, one of the questions I am frequently asked by my clients, is what blood tests they should have to measure their nutrient levels. Most appear disappointed when I tell them that there are very few nutrients for which we have tests that accurately assess the adequacy of their intake, and body stores. Iodine is no exception.
As mentioned above, the major route of excretion of iodine is via urine, and the kidneys excrete a fairly fixed proportion of the amount of dietary iodine that has been absorbed. Hence, the most widely accepted method for assessing iodine status involves measuring urinary iodine concentration. The most frequently used test is the spot urine iodine, a one-off measurement of the amount of iodine excreted in the urine. The 24-hour sample involves, as the name implies, measuring the amount of iodine excreted in a day's worth of urine. But these tests were developed to assess population-level iodine nutriture, not the adequacy of iodine intake in an individual. Here's the background:
"A landmark study was published in 1970 which presented data from 186 areas and over 3000 people with goitres in Central America.41 The authors measured urine iodine and creatinine, and estimated the 24-h excretion of iodine based on these values. They observed that goitre was endemic (defined as a prevalence of greater than 10%) in all areas where the mean estimated 24-h urine iodine excretion was less than 25 μg, in most of the areas where it was 25–49 μg, in a third of areas where it was 50–99 μg and in no areas where is was greater than 100 μg. It is upon these observations that the WHO bases their cut-off values for UI [urinary iodine] concentration.
The WHO advises that a median UI concentration of greater than 100 μg/L indicates population iodine sufficiency.42 This is the most widely used indicator of population iodine status and is considered to be reliable in the context of school-aged children. The most appropriate cut-off to use for adults in this situation is not clear, although some authorities suggest 60–70 μg/L.34" [emphasis added]
The assessment of iodine status – populations, individuals and limitations
OK, so why isn't urinary iodine an accurate measure of iodine status in individuals? Because urinary iodine concentration reflects only recent dietary intake. If I ate a high-iodine meal today, my urinary output of iodine would be high for a few hours afterward, and then it would slowly drop off again. If I sent multiple spot urine samples taken throughout that day off for analysis, they would all yield different results as my renal excretion of iodine rises, peaks and falls. Then if all my meals for the next three days were low in iodine, my urinary iodine excretion would be lower than on the high-iodine meal day, whether measured by spot or 24 hour collection. So which test result should I use as an indicator of my iodine status, and whether I should be increasing or decreasing my dietary intake?
But wait, it gets even more complicated. It turns out that there are both circadian and seasonal fluctuations in urinary iodine excretion:
"One study performed in Switzerland in the mid 1990s looked at UI concentrations in spot samples in 1729 volunteers.44 The authors observed significant seasonal variation in UI concentration in children with differences of between 5 and 30% in mean values between summer and winter, with values being higher in the summer months. They attributed this principally to known differences in cow’s milk iodine concentration, and differences in milk consumption. A further more recent study investigated this seasonal effect in 401 healthy adults living in Belgium.45 They too observed that UI concentration varied significantly with the seasons, and this difference persisted after controlling for age, sex, ethnicity and BMI. There was a greater proportion of individuals with a UI concentration less than 100 μg/L in the winter than there was in the summer.
There is also evidence that variation in iodine excretion may follow a circadian rhythm. A study from Switzerland looked at over 3000 spot samples from 42 adults and children over the course of two years and uncovered circadian rhythmicity that was independent of season, age and gender.46 They observed that UI concentration is lowest at 0800–1100 h, and increases progressively between 1200 and 0000 h and that concentrations generally peak 4–5 h after meals. They concluded that studies using spot urine samples from fixed times of the day such as the morning could not be reliably compared with studies where sampling occurred at different times of the day or where sampling times were not fixed."
The assessment of iodine status – populations, individuals and limitations
When urinary iodine excretion is measured in hundreds to thousands of people, the law of large numbers kicks in, essentially evening out this natural variability so that some useful information about population iodine status can be gleaned. However,
"There is currently no clear consensus on the most appropriate way to use urine iodine measurement to assess iodine status in an individual, or even whether this is in fact a useful thing to do. However, it is clear that one cannot simply use the WHO endorsed cut-off of less than 100 μg/L from a single-spot urine as this figure refers to a population median."
The assessment of iodine status – populations, individuals and limitations
In a nutshell, applying ranges developed to assess iodine status in populations, to individuals, will lead to overdiagnosis of iodine deficiency. And that overdiagnosis will almost certainly result in overtreatment, such that people who don't actually need iodine supplements will take them, putting at least some of them at risk of overdose.
Could repeated testing be a solution to the problem of measuring iodine status in individuals? A team of very determined Danish researchers studied urinary iodine excretion in 16 healthy males who were living in an area of mild to moderate iodine deficiency, and determined that "in order to achieve a precision range ± 20% for an individual, 12 spot urine samples are required, or 7 spot samples with an iodine to creatinine ratio to calculate estimated iodine excretion." Swiss researchers confirmed these results with a slightly larger sample size (22 healthy females), and "concluded that a minimum of 10 repeated spot urine samples are required to achieve a precision of 20%". That's a lot of testing, which is not only cumbersome but expensive, given that the cost of these tests is not covered by Medicare. (For my overseas readers, Medicare is Australia's universal health insurance scheme.)
Beyond the cost and time burden, there's the issue of whether we're measuring the right thing:
"It is crucial to consider whether or not urine iodine excretion in an individual, regardless of the precision of measurements, is actually truly reflective of individual iodine status in a way that is clinically meaningful. The thyroid gland is able to store large quantities of iodine; it is known that 70–80% of the body’s total iodine stores, comprising 15–20 mg, are found within the thyroid.51 These stores are unaffected by short-term changes in iodine intake, and urine iodine excretion is predominantly a measure of recent iodine intake as the vast majority of iodine absorbed by the gastrointestinal tract is excreted within 24–48 h.52 Therefore, any form of urine iodine measurement is unlikely to be useful in determining whether or not an individual is iodine deficient unless samples are collected over a prolonged period of time, which will severely limit the clinical utility. Additionally, sampling would ideally cover a sufficiently long period of time to account for seasonal variations in intake of iodine, and this is clearly beyond the realms of routine clinical practice."
The assessment of iodine status – populations, individuals and limitations
Well, that's a bummer.
So what in the bloody hell should I do?
If you've made it this far, you're probably feeling both worried and confused. Too little iodine is bad for you; too much iodine is bad for you; if you're iodine-deficient during pregnancy, your baby could be born stupid; and it's next to impossible to accurately determine your own iodine status. Believe me, both as an individual and a practitioner committed to helping my clients achieve optimal health, I feel your pain.
Here's what I personally do, since I don't eat commercially-produced bread or use salt in my cooking:
I eat seaweed - nori, dulse or wakame, but not kombu - three times per week.
I use a seaweed-based liquid fertiliser on my vegetable garden and fruit trees, to make sure my home-grown produce contains iodine.
If you do use salt in your cooking and/or at the table, you should use iodised salt as even if you live in an iodine-replete region, you won’t ‘overdose’ on iodine from this source.
And if you buy commercially-produced bread, you need to know that bread labelled as organic is exempt from mandatory fortification with iodine.
For my female clients who are intending pregnancy, or already pregnant or breastfeeding, I recommend taking a 150 μg iodine supplement each day as well as consuming nori, dulse or wakame three times per week.
Those who live in the southeastern States (New South Wales, Victoria and Tasmania) may want to consider eating seaweed more frequently, or using a 200-250 μg iodine supplement, especially if they don't eat commercial bread or use iodised salt, and most especially if pregnant or breastfeeding. The populations of these States had a suboptimal average urinary iodine excretion prior to the introduction of mandatory iodine fortification of bread, whilst Queenslanders and Western Australians were in the optimal range. And even after that program was implemented, pregnant Tasmanian women who were not taking an iodine supplement were still found to be below the optimal average urinary iodine concentration.
My non-Australian readers can check their local health authorities (uggh, I hate that word) for information on population iodine adequacy in their region.
If you really, really want to test your iodine status, the 24-hour urine collection is somewhat more useful than the spot iodine test, but you still need to take the results with a grain of (hopefully iodised) salt.
And finally, stay the hell away from kelp supplements, Lugol's solution and other high-iodine preparations. Remember the Goldilocks principle: not too little, not too much, but just the right amount.
This post has taken approximately 15 hours to research and write. If you feel you’ve obtained value from reading it, please consider a paid subscription:
I have Morgellons and high dosage iodine supplements in the form of SSKI and Lugol's solutions have been promoted as a "cure", though I know no one who was actually "cured". Instead SSKI and Lugol's did inhibit the skin extrusions of Morgellons sometimes for long periods though when discontinued, Morgellons visibly returned.
I knew this was likely a dangerous protocol but your article has confirmed my layman's thoughts. Now I know what to say to other Morgellons sufferers.
Thank you, Robyn, and, yes, iodine has never been so interesting. Thank you for your great work.
God Bless.
Very interesting comments of yours below. And, I objectively agree with what you are saying. Iodine, *like other supplements*, can/do bite i.e., make a person feel worse. I have a few examples of folks I know who've been bitten by Lugol's and other iodine sups. Too long to get into here.
Your advice on how to get more iodine 'the right way' is right on, too. Good job, per the norm for you. Common sense and staying as objective as possible.
________________________________________
Robyn:
• "And finally, stay the hell away from kelp supplements, Lugol's solution and other high-iodine preparations"
• "In any case, Lugol's is not intended for use as an iodine supplement …… "