
Get stronger, live longer
Survival of the strongest

I’ve written several articles about the benefits of maintaining a strong, muscular body as one gets older, for easing the menopausal transition (Muscle up to beat hot flushes), maintaining cognitive sharpness (Strong body, healthy brain) and preventing dementia (Lean body, healthy brain).
So it’s a source of enormous frustration to me, that one of the most challenging tasks that I regularly face as a Lifestyle Medicine practitioner is getting my clients - especially the middle-aged females, and practically all the older folk - to implement an effective strength training program. Most of my clients in these demographics think that aerobic activities such as walking, cycling and swimming are all they need to do to stay healthy. But people can be aerobically fit yet undermuscled.
Some loss of muscle mass is inevitable with age, but if you’re not doing any exercise that specifically strengthens your muscles, you’re going to lose mass and strength at an accelerated rate that puts you at much higher risk of falls, fractures, and cognitive decline.

For those of you who haven’t got the memo yet that muscle strength is the golden key to living longer - and actually enjoying it - a new study has found that older women with greater muscular strength had significantly lower mortality than weaker women, even when they weren’t particularly physically active. And the relationship was linear, meaning that each incremental increase in muscle strength was associated with an incremental decrease in mortality risk.
The study was conducted in 5472 women aged between 63 and 99, who were enrolled in the Objective Physical Activity and Cardiovascular Health in Older Women (OPACH) study, an ancillary study to the long-running Women’s Health Initiative (WHI).
Upon enrolment, the women were fitted with an accelerometer for one week to track their steps, performed a timed walk test to assess cardiorespiratory fitness, and underwent blood tests and measurement of height, weight and blood pressure.
They also took two tests of muscle strength, which were the particular focus of this study:
Dominant hand grip strength, measured in kg using a dynamometer;
Time taken to complete five unassisted chair stands.
A hand dynamometer is a device that you squeeze as hard as you can to measure your grip strength, as shown below. Participants’ grip strength ranged from less than 14 kg in the weakest group, to more than 24 kg in the strongest.

Unassisted chair stands involve sitting down on a chair and standing up again as fast as you can, without using your hands or arms for assistance. The slowest group took more than 16.7 seconds to perform five of these, while the fastest took less than 11.1 seconds. Time yourself using a stopwatch, to see how long it takes you!
During an average follow-up time of just under eight-and-a-half years after this initial testing, 1964 of the 5472 participants (35.8 per cent) died - not a big surprise, given that the average age at enrolment was 78.7 years.
But the women who either had greater grip strength and/or faster sit-to-stand time at baseline, had a significantly lower risk of dying, even after adjusting for age (older people are obviously more likely to die than younger people), race and ethnicity (black and hispanic women had stronger grip strength than white women, and black women were also faster on assisted chair stands).
Check out the Kaplan-Meier survival curves below. Most of the strongest participants are still alive at the 11-year mark, while the majority of the weakest are dead:
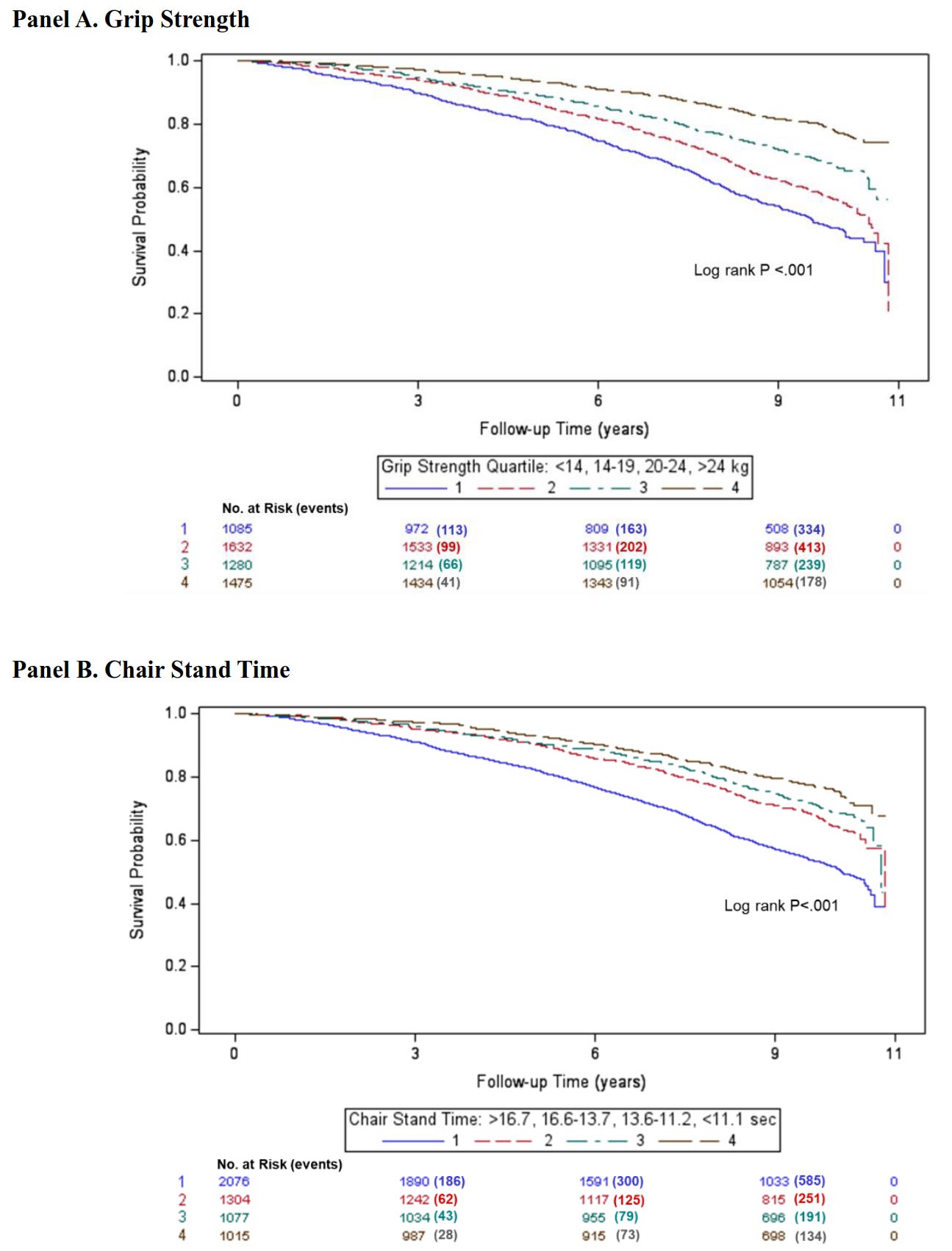
Even after statistical adjustment to account for potential confounding by sociodemographic factors, lifestyle behaviours, and comorbidities that might lead to both decreased muscle strength and a shorter life expectancy, the inverse relationship between muscle strength and lower mortality persisted.
The researchers also examined the relationship between muscle strength, physical activity level and mortality. In the case of grip strength, it made no difference whether participants met the minimum recommended levels of aerobic activity or not - muscularly stronger women lived longer, either way.

Terminal illnesses such as cancer and heart failure cause a loss of muscle mass. To rule out the possibility that the study’s results were skewed by reverse causation - the inclusion of women who were weak because they were close to death at enrolment - the researchers conducted separate analyses that excluded all deaths that occurred in the first three years, and the first five years, of the study… and still, the relationship between muscular strength and mortality persisted.
Interestingly, the correlation between grip strength and chair stand time was very small, meaning that participants could have high grip strength but slow chair stand times, and vice versa. The researchers speculated that “the 2 measures are largely assessing different constructs”, and this is highly likely.
For starters, grip strength reflects upper body strength while the chair stand measures lower body strength. And furthermore, there’s a difference between strength - how much force your muscles can produce - and power - the amount of work performed over a given time period (also known as explosive power). The dynamometer measures strength, while the chair stands estimate power (and endurance).
The authors’ conclusion encapsulated the study results nicely, as well as highlighting the need to provide specific guidelines to help older people regain and maintain muscle strength:
“In this cohort study of ambulatory women aged 63 to 99 years, higher skeletal muscle strength was associated with significantly lower all-cause mortality. This association was evident after controlling for several strong mortality risk factors and in women not meeting aerobic activity guidelines. Our finding supports current national recommendations that promote participation in muscle strengthening activity for optimal aging and longevity. To improve guideline recommendations, future research should better characterize the type and amounts of muscular strengthening activity associated with more specific outcomes across the health span.”
Muscular Strength and Mortality in Women Aged 63 to 99 Years
How to get started with strength training
When I’m working with older clients who have never done strength training, I encourage them to begin with simple body weight exercises such as squats - using a chair or wall for balance - and push-ups against a wall or kitchen bench. If even these movements are challenging due to injuries or joint problems, it’s well worth consulting an exercise physiologist to design a tailored strength-training program, commencing with improving joint function.
Resistance bands are an incredibly useful tool for strength training, suitable for both beginners and more advanced exercisers. Even people who are bed-bound or chair-bound by illness or injury can use resistance bands, if they have someone to assist them with attaching the bands to suitable anchor points.
The next step up is weight training equipment such as dumbbells, barbells, kettlebells, sandbags and weights machines at the gym. Most older people need instruction in using this equipment safely; as one of my clients - a man in his mid-nineties - explained to me recently, when he was young, only freaks and weirdos worked out at the gym!
Some of my older female clients believe that regular yoga is all they need to do to stay strong. Yoga offers many benefits, but it’s not effective at building and maintaining muscle mass as we age. For that, you need to make your muscles work against resistance, and that resistance needs to be progressive - that is, as it gets easier to do an exercise, you make it harder by increasing the number of repetitions, increasing the weight, or both.
‘But I’m too weak to even begin strength training!’
It might sound daunting if you’ve never done it before, but the most common thing I hear from my older clients once they finally psych themselves up to engage in regular strength training, is how much they enjoy watching themselves get stronger every week. It really is a buzz to observe how quickly your body responds to strength training, even when you’re badly deconditioned. My elderly Mum, who has to use a walker after fracturing first her pelvis, and then her femur, loves to brag about how many bicep curls and overhead presses she can do at her seniors exercise class!
And if you want proof that no one is too out-of-shape to start strength training, check out this study in which ten frail nursing home residents aged in their 80s and 90s undertook an eight-week training program which consisted of doing just three sets of leg extensions, three times per week. Seven of the ten participants had osteoarthritis, six had coronary artery disease, six had suffered an osteoporotic fracture and four were hypertensive. Not exactly the dream team!
One poor chap had to drop out of the study due to strain at the site of a previously-repaired hernia, but of the remaining nine, all had significant lower body strength gains by the end of the program (averaging a three- to fourfold increase), and muscle area increased in five of the seven who had before-and-after CT scans
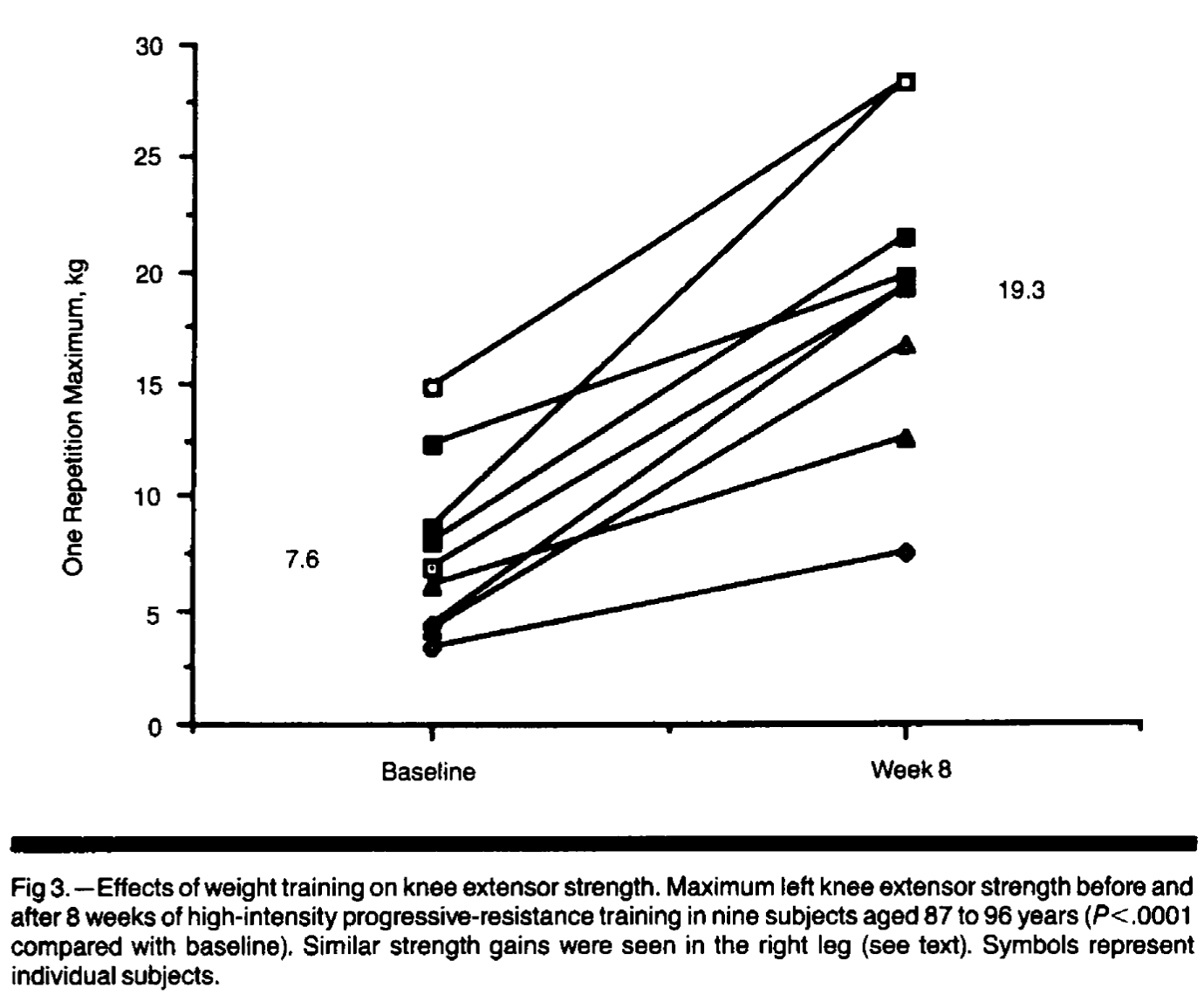
That’s cool, but what’s even more impressive is the impact that this simple training program had on participants’ mobility:
“Changes in functional mobility accompanied the improvements in muscle strength and size. Although habitual gait speed did not change significantly with training, in the five subjects who completed the tandem gait assessment at both time points, there was a decrease in walking time, from 43.4 ± 25.7 to 29.6 ± 22.4 seconds (P=.05, one-tailed paired t test). This represents a 48% improvement in tandem gait speed, from 13.8 cm per second to 20.4 cm per second. Two subjects no longer used canes to walk at the end of the study. One of three subjects who could not initially rise from a chair without use of the arms became able to do so.”
The researchers concluded,
“The favorable response to strength training in our subjects is remarkable in light of their very advanced age, extremely sedentary habits, multiple chronic diseases and functional disabilities, and nutritional inadequacies. The relationship we observed between muscle strength and fat-free mass suggests that preservation of fat-free mass, whether through activity or nutritional intake, is an important determinant of muscle strength in very old age. We hypothesized that disuse atrophy was the major contributor to the muscle dysfunction in these nursing home residents and that without altering any of the other factors, some reversal of the muscle weakness and atrophy would be possible. Our findings suggest that a portion of the muscle weakness attributed to aging may be modifiable through exercise.”
Sadly, when the program ended and participants went back to their sedentary ways, their progress rapidly reversed:
“A significant 32% loss of maximum strength was seen after only 4 weeks of detraining.”
If you don’t use it, you really will lose it.
And if you want to ditch Substack and get my posts straight from the source - as well as commenting and viewing any content that Substack won’t let you see without using their privacy-invading facial recognition app - just
I am a 76 year old male and did the chair rises in 10 seconds. I do a bit of working out with lighter dumbbells. A few years back I used heavier dumbbells and would work up soreness in my shoulders and back. Then it would take weeks before I could get back to using them.
Anyway, this idea of muscle strength is intriguing and for sure my nearly 80 year old wife would likely benefit. She has had several operations in the last 9 months for a hernia and bowel obstructions, the latest being a few weeks ago. Once she is fully recovered, I hope to help her get back to being more mobile.
Thanks for the information. It will be very useful.
Having chalked up my three score years and ten on the biological clock, I know only too well the reality that muscle mass declines with age. I used to be able to power away doing repeated hill sprints against high resistance on an exercise bike but, although the spirirt is still willing, the leg muscle strength isn’t. Still, some moderation of expectation allows me to cope with that.
For the upper half of an ageing body, the story is similar. After wasting three decades as a distance runner who totally ignored my pencil-thin arms and the rest of the upper body equipment, chronic overuse running injuries forced me to do more gym classes like circuits and boxercise classes and some weight machines which improved things a lot. These days, I have added a set of dumbells and resistance bands to my home gym to keep it up, although that pesky age-related muscle mass decline is manifesting itself upstairs, too.
What I used to be able to do when I was 20, or 30, or even 40, is not what I am capable of doing now I am 70 but that’s life – we aren’t going to last forever.
My five unassisted chair rises, I’m pleased to be able to boast, were completed in 12 seconds, for what it’s worth – and that includes with that old man’s issue of a hernia repair (another occupational risk factor of ageing).
Thanks for the detailed article.