


Who's killing Grandma, really?

As the war rhetoric ramps up against those who are exercising the right to decline an experimental medical treatment that is guaranteed to us by the Declaration of Helsinki, the unvaccinated are being blamed for the emergence of vaccine-resistant variants such as the now-dominant Delta strain of SARS-CoV-2.
The rise of vaccine-resistant strains is acknowledged to be an impediment to Australia’s attainment of herd immunity – a situation in which a sufficient proportion of the population has sterilising immunity to an infectious agent to prevent the spread of that agent through the community. (Sterilising immunity means that an individual cannot become infected by a pathogen such as a bacterium or virus, nor pass it on to others.)
And if herd immunity is not attained, the small percentage of the population which is susceptible to serious illness and death from SARS-CoV-2 infection (mostly the infirm elderly and younger people with immunosuppression, obesity or other comorbidities) remain at risk.
The argument that the unvaccinated are driving the development of vaccine-resistant viral strains and thus preventing the attainment of herd immunity is absurd on its face, but let’s lay out the facts systematically, for the hard of thinking.
Fact #1: Vaccination is a form of selection pressure which favours the emergence of immune escape variants such as the Delta variant
The fact that vaccines push pathogens to mutate in ways that allow them to evade vaccine-induced immunity has been known for many years, as I pointed out in a previous article, Why Australia’s COVID-19 exit plan can’t succeed – Part 2.
To reiterate an important point from that earlier article, if a vaccine is leaky – that is, it induces an immune response that reduces the growth rate and/or toxicity of the pathogen but does not block infection – it will actually select for mutations that make the pathogen vaccine-resistant.
These vaccine resistant strains are called immune escape variants, and their rise was predicted by Geert Vanden Bossche back in March 2021.
Vaccine-resistant mutations may well spontaneously arise in the body of an infected unvaccinated person along with other mutations, but since they have no particular survival advantage over other random mutants, they will not become the dominant strain within that individual’s body. Only in the bodies of vaccinated individuals do vaccine-resistant strains enjoy a competitive advantage over other strains, allowing them to become dominant.
And it’s those vaccine-resistant strains that pose the real threat to Grandma.
Fact #2: Vaccine-resistant strains become more dominant as the vaccination rate rises
This fact logically follows from the first, but it’s worth illustrating it graphically:
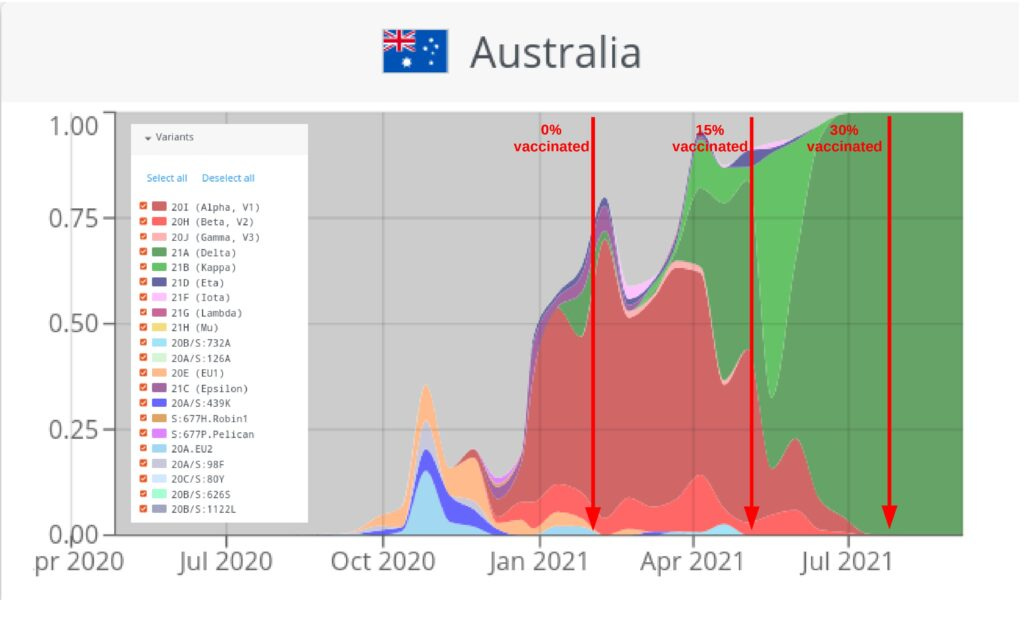
Data sources: CoVariants.org and Our World in Data
As can readily be seen, before the COVID-19 vaccine rollout began in Australia, there was a diverse range of variants of SARS-CoV-2, with the Alpha variant (which was not vaccine-resistant) being the most prevalent variant sequenced.
By the time 15% of the population had received at least 1 injection, the Alpha variant had declined in prevalence and the vaccine-resistant Delta had sharply increased. And by the end of July, when 30% had received at least 1 dose, Delta was for all intents and purposes the only strain of the virus left in circulation.
And that means that if Grandma gets exposed to SARS-CoV-2, it’s almost certain to be the Delta (vaccine-resistant) strain of the virus.
Fact #3: Vaccine-resistant strains reduce the protection afforded by the vaccine to those who are in most need of it
The vast majority of people who contract SARS-CoV-2 will either experience no symptoms at all, or a mild to moderate flu-like illness.
They have little to no need of any vaccine for personal protection, especially if they adopt rational fever-management practises and familiarise themselves with evidence-based early treatment protocols to use in the unlikely event that they develop COVID-19.
These low-risk individuals are being emotionally manipulated to accept an experimental injection in order to “protect the vulnerable”.
But as explained above, the higher the percentage of the population that is vaccinated, the more dominant the vaccine-resistant strains of the virus become. Once again, Granny is now more likely to be exposed to a vaccine-resistant strain of the virus, which will evade her vaccine-induced antibodies.
Fact #4: Vaccinated people who become infected with SARS-CoV-2 are more likely to shed vaccine-resistant variants of the virus
It is now beyond dispute that vaccinated people who become infected with the Delta variant of SARS-CoV-2 have just as high a viral load as unvaccinated people, and therefore are just as likely to be as infectious to others.
However, given the selection pressure exerted on the virus by vaccine-induced antibodies, more vaccine-resistant virus develops in and is shed by these vaccinated “breakthrough” cases.
Watch out, Granny!
Fact #5: Vaccinated individuals are more likely than unvaccinated individuals to become ‘Typhoid Marys’
Now that politicians and medical bureaucrats have been forced to admit that COVID-19 jabs don’t prevent infection or transmission, they’ve switched their sales pitch. Sure, they tell us, the shot won’t stop you getting infected, but it will keep you out of hospital.
Just think about that for a minute. If you develop a breakthrough infection but don’t feel sick, you’re more likely to go about your daily life, merrily shedding virus from your airways as you do so. And if you happen to live with, visit, or work amongst frail elderly people or at-risk younger people, you could easily infect them with vaccine-resistant viral variants.
Meanwhile, if it’s true that the unvaccinated will be far more likely to develop symptoms if they’re infected, those symptoms serve as their warning to stay well away from vulnerable people… including Granny.
Fact #6: Vaccination delays the development of herd immunity, causing vulnerable people to be at risk for longer
As the world-renowned epidemiologists who signed the Great Barrington Declaration tried to explain back in October 2020, attempting to suppress the spread of SARS-CoV-2 via policies such as lockdowns, stay-at-home orders and school closures delayed the development of herd immunity that would otherwise have allowed vulnerable people to resume normal participation in life, with minimal risk of infection.
Without lockdown, they estimated herd immunity may have taken only 3-6 months to develop. But here we are, 18 months into the global pandemic with no end in sight.
Population-wide vaccination programs have further delayed the development of herd immunity because they have resulted in more transmissible variants that escape vaccine-induced immunity.
Even Andrew Pollard, the head of the Oxford Vaccine Group which developed the AstraZeneca jab, has acknowledged that vaccine-induced herd immunity is “not a possibility” due to the (vaccine-induced) emergence and rise to dominance of the Delta variant.
The chief epidemiologist of Iceland (which has vaccinated 82% of its population, 80% with 2 jabs) has admitted that herd immunity can only be achieved by allowing the virus to spread throughout his small island nation, while attempting to shield the most vulnerable from it.
But how can Granny be shielded when all her caregivers have been injected with a product which turns them into perfect superspreaders if they contract SARS-CoV-2: asymptomatic or so mildly symptomatic that they don’t realise they’re infected, but carrying a high viral load of vaccine-resistant virus?
Fact #7: Only natural infection can facilitate herd immunity to SARS-CoV-2
All people of good will wish to protect the vulnerable. Just about all of us have a “Grandma” in our lives – either a frail elderly person or a younger person suffering from immunosuppression or serious illness that raises their risk of getting seriously ill from a SARS-CoV-2 infection.
The only way we’re ever going to be able to protect these people is to attain herd immunity.
And only natural infection confers the robust, broad and durable protection against infection and transmission of SARS-CoV-2 that is necessary for herd immunity to develop.
Let’s hope that by the time the politicians and medical bureaucrats wake up to this undeniable fact, we’ll still have enough unvaccinated people left to get there.