
Psychedelics vs antidepressants
There's a lot of hype around psychedelic-assisted therapy, but a new study has poured cold water on it.

Back in April 2023, I wrote a post - Psychedelics - panacea or psychiatry's new shiny object? - expressing my concerns about the burgeoning movement to promote the use of psychedelic drugs for treatment of depression, PTSD and other manifestations of psychological distress. Those concerns include:
The absolute centrality of correct set, setting and post-trip integration to achieving positive outcomes from psychedelic-assisted therapy, and the difficulty in ensuring that all patients receive these;
The high prevalence of ‘bad trips’ even in carefully-screened participants taking part in well-managed clinical trials;
The danger of therapy abuse, which is substantially heightened in the context of profoundly mind-altering substances;
The potential for inculcating beliefs and attitudes during psychedelic sessions, that could be personally or socially destructive;
The vigorous promotion of psychedelics by venture capitalists and pharmaceutical companies who, one can safely assume, are motivated not by beneficence to suffering humanity, but by the prospect of healthy profits, which are contingent on expanding the market for their products;
Reinforcement of the ‘pill for every ill’ mentality, rather than addressing underlying drivers of depression and other states of psychological distress;
Lack of understanding of how psychedelics actually work, and what ‘working’ means - that is, how psychedelics change the brain, and what the medium- to long-term implications of these changes are;
Following on from the previous point, the fact that we have no long-term follow-up studies on the outcome of psychedelic-assisted therapy, with the longest follow-up period so far being just six months; and
The failure of psychedelics to deliver on the promise of ‘curing’ depression in just one or two sessions, with many people converting to long-term use.
Despite these concerns, I was, at the time, cautiously optimistic that psychedelic-assisted therapy may turn out to be safer and more effective than any of the antidepressant drugs currently in use.
But a study published in the latest edition of JAMA Psychiatry has torpedoed those faint hopes. It turns out that when comparing open-label studies of antidepressant drugs (that is, studies in which participants know that they are receiving a drug, and not a placebo), with either open-label or blinded studies of psychedelic-assisted therapy, psychedelic-assisted therapy is no more effective at relieving depression than conventional antidepressants.
The authors identified sixteen open-label trials of various types of antidepressants for the treatment of major depressive disorder, and eight trials of psychedelic assisted therapy of which six were formally blinded and two were open-label. Seven of these eight trials used psilocybin and the eighth used ayahuasca.
They used data from these trials to test three hypotheses:
That psychedelic-assisted therapy would be more effective than antidepressants administered in an open-label setting, and that the difference between the two forms of treatment would be clinically significant, not just statistically significant.
That open-label antidepressants would be more effective than antidepressants administered in a blinded trial, and that the difference between open-label and blinded trials would be clinically significant.
That there would be no clinically significant difference in outcomes between blinded and open-label trials of psychedelic-assisted therapy.
The forest plot below tells the tale:
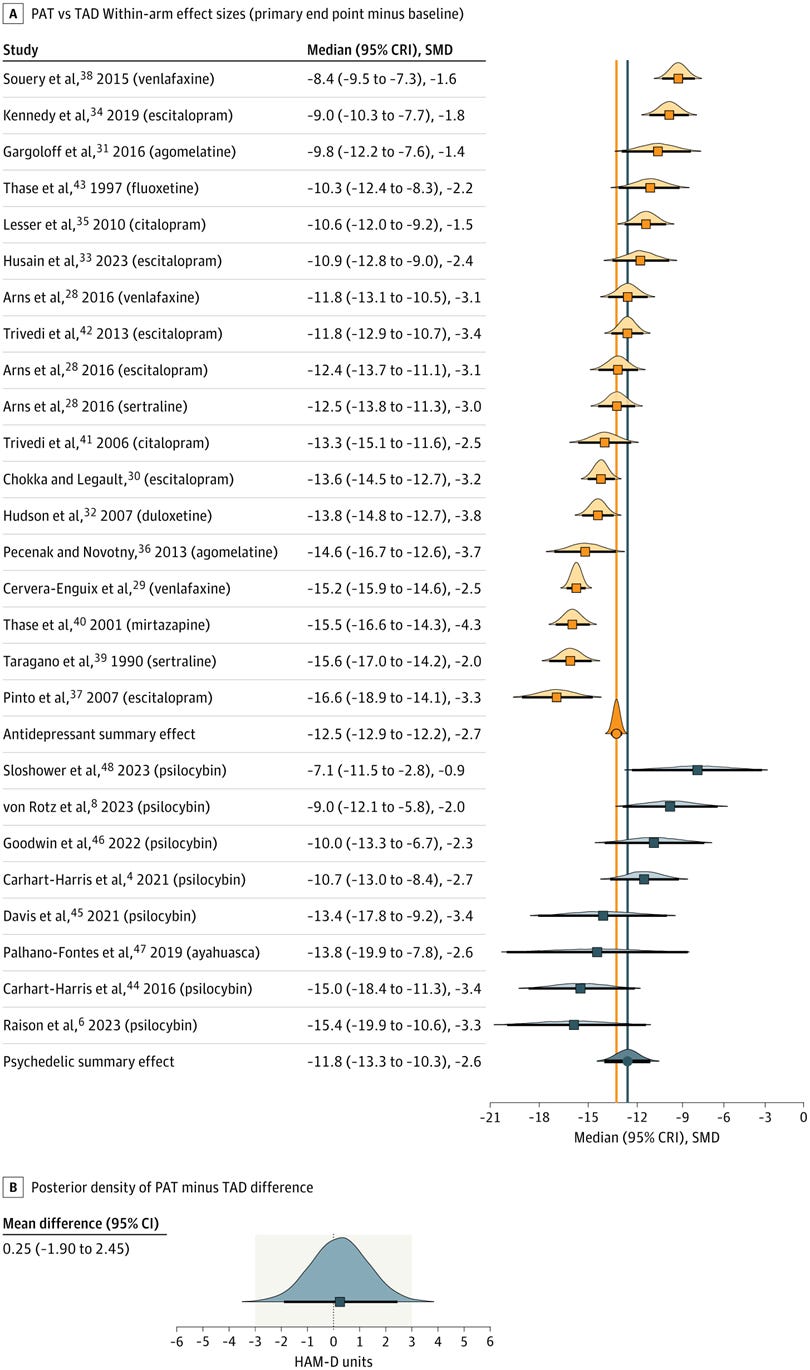
For those unfamiliar with reading a forest plot, the orange and blue squares represent how much change there was in participants’ depression scores on a standardised scale (the 17-item Hamilton Depression Rating Scale [HAM-D]) by the end of the study; the lower the score, the greater the improvement. A decrease of three to five HAM-D units is considered the minimal clinically important difference, i.e. an improvement in depressive symptoms that is large enough to make the patient’s life better. The orange and blue vertical lines indicate the average effect of antidepressants and psychedelic-assisted therapy, respectively.
Part B of the figure shows that the difference between the two treatments was negligible, amounting to approximately 0.3 HAM-D units. Antidepressants turned out to be slightly more efficacious than psychedelics (although the difference was not clinically significant), contradicting the authors’ hypothesis that in unblinded conditions, psychedelics would outperform antidepressants.
How could this be? In randomised double-blind placebo-controlled trials, antidepressants arguably aren’t any better than placebos at alleviating depressive symptoms; the best-case scenario is that antidepressants may outperform placebo by 1.75 to 2.4 points on the HAM-D, which is below the threshold for minimum clinically important difference. Psychedelic-assisted therapy, on the other hand, substantially outperforms placebo, by an average of 7.3 HAM-D units.
Ah, but you see, placebos themselves are tricksy little things. We’ve all heard of the placebo effect, which is most concisely defined as “the form of a treatment without its substance”, and slightly more elaborately as “any treatment deliberately used for non-specific psychological or psychophysiological effect”.
Participants in double-blind placebo-controlled trials of antidepressants are often able to correctly deduce whether they’ve been given the active treatment or a placebo, usually because of the presence or absence of drug side-effects. This is called functional unblinding. Trial participants who guess that they have received the drug, rather than placebo, experience positive expectancy - the expectation that they will get better. Conversely, participants who guess that they have received placebo experience the ‘know-cebo’ effect - the disappointment that they did not get the drug, which creates negative expectancy.

63 per cent of participants in blinded antidepressant trials correctly guess their treatment allocation to drug or placebo. Comparing open-label with blinded trials of antidepressants, the authors found that open-label administration was associated with slightly better outcomes than blinded treatment, but the difference was not clinically meaningful (approximately 1.29 HAM-D units). The authors attributed the slight superiority of open-label antidepressants to positive expectancy - that is, all participants knew that they were receiving active treatment, so they all expected to get better.
Conversely, patients in blinded psychedelic trials can almost always tell whether they have been given a placebo or the active drug, even when an active placebo is used, such as niacin, which induces intense flushing but no hallucinations or other unusual psychological phenomena. Unsurprisingly then, the authors found no difference in outcomes between blinded and open-label psychedelic-assisted therapy trials, because all such trials are effectively functionally unblinded.
Furthermore, the response to placebo is much lower in trials of psychedelic-assisted therapy than in other treatment modalities (equivalent to 4.0 HAM-D units of difference) because of the know-cebo effect. Participants who were hoping to receive a psychedelic drug that will induce intense mystical experiences, leading to a profound psychospiritual transformation, feel pretty bummed out when they realise they got a placebo that does diddly-squat other than giving them temporary hot flushes. And in fact, placebo recipients in controlled trials of psychedelic-assisted therapy often deteriorate, whereas placebo recipients in antidepressant trials get better over time:
“~55% of PAT[psychedelic-assisted therapy]’s between-arm effect is explained by the lack of improvement in the placebo arm. In some psychedelic trials, depression worsened in the placebo group.57,58 In contrast, the most comprehensive meta-analysis of TAD [traditional antidepressant] trials involved 304 placebo groups, and patients improved in all 304 of them.”
So that 7.3 HAM-D unit superiority of psychedelics over placebo that we see in randomised controlled trials, is largely due to a suppressed placebo effect, rather than to psychedelics being a more effective treatment for depression than antidepressants which only outperform placebo by about 2 HAM-D units.
And what was that about depressed patients getting better while taking placebos? Let’s have that one again, shall we?
"The most comprehensive meta-analysis of TAD [traditional antidepressant] trials involved 304 placebo groups, and patients improved in all 304 of them."
It’s almost as if depression is a normal and natural response to life’s setbacks, and most people recover from it without the need for any ‘treatment’ at all, after they have worked through the setback in their own fashion. Wait, didn’t I write exactly that in The depression misconception? Why yes, as a matter of fact, I did!
What this study tells us.. and what it doesn’t
To sum up, contrary to the hype, psychedelic-assisted therapy with either psilocybin and ayahuasca isn’t any better at relieving the core symptoms of depression than open-label antidepressants, and in fact, is slightly inferior, although the difference is not clinically meaningful.
It’s important to note that only studies using psilocybin and ayahuasca fulfilled the inclusion criteria for this study, so we don’t know whether other psychedelics, such as MDMA and DMT, might be more effective.
Also, psychedelic-assisted therapy may lead to improvements that aren’t captured by the Hamilton Depression Rating Scale. The Hamilton scale measures rather prosaic indicators such as changes in mood, sleep habits, feelings of guilt, psychomotor retardation (slowed movements and thinking) and ability to perform one’s normal work and activities. Psychedelic-assisted therapy aims to facilitate profound shifts in how participants see themselves in relation to their life experiences, the people they’ve encountered, and their deeper place in the ‘big picture’ of life - insights that are not captured by a 17-item questionnaire.
And summed measures of clinical effects don’t capture the individual experiences of people. Some individuals may experience profound benefits from a therapy that does not appear to be effective in the aggregate. But conversely, some people may experience great harms.
But at the end of the day, no one becomes depressed because of a deficiency of psychedelics. As I discussed at length in The depression misconception, depression is failure feedback - the predictable, functional and adaptive response to failure to achieve one’s life goals, whether that failure is due to actions taken by oneself, or to the slings and arrows of outrageous fortune. If psychedelics, psychological therapy, or the combination of the two, help people to accurately identify the source of their problems, and to develop and implement effective plans for solving them, then they will be successful in treating depression. The question is, do we really need psychedelics to achieve these goals, or are they just psychiatry’s latest shiny new object?
And if you want to ditch Substack and get my posts straight from the source - as well as commenting and viewing any content that Substack won’t let you see without using their privacy-invading facial recognition app - just
Drugs...legal, illegal or otherwise never cure anything. Maybe you take a drug and manage something but cease the drug use and the problem is still there. The goal should be to remove as many toxic disruptions as you can. Things like vaccines, drugs, fake foods, smoking, alcohol, chemical poisons in your environment and stress factors. The idea of continually adding toxic or poison things into your world to fix problems is ridiculous.
"Trial participants who guess that they have received the drug, rather than placebo, experience positive expectancy - the expectation that they will get better. Conversely, participants who guess that they have received placebo experience the ‘know-cebo’ effect - the disappointment that they did not get the drug, which creates negative expectancy." I taught Ethology (a branch of Ecology/ Animal Behavior), at Univ, where the critical premise of the entire field of study is the subject CANNOT know they are being watched/studied or their behavioral responses are completely, and scientifically biased (as you very rightly point out!). There are thousands of studies that prove this scientific fact. You thus use that field in this post (and your notes) to argue against the study of "falsified behaviors" and the fake drugs shrinks use to "cure" them. The shrinks fought Conrad Lorenz when he introduced the Ethology field about 90 years ago. The shrinks won, so what we now have are high rise hotels in NA filled with hundreds of shrinks giving dangerous, useless drugs, destroying their "patients'" brains, sometimes for life, only for the shrinks' money! This is even outlined in the Merck MD manual that names the fake drugs that are still used every day by almost all the shrinks. Your post and notes really make you sound like an Ethologist to me, well done! The shrinks (some working on their shrink PhDs) in my course all got C and D's, especially the ones that had shrink practices. All their exam answers were glorified BS! No doubt as a Naturopath you use vitamins to do what shrinks fake. Personally, I used vitamins to eliminate all sleep problems caused from COV morons, that killed my father, mother, brother, aunt, and cousin with their fake, "unsafe and ineffective" vax. I received their illegally-altered death certificates, "natural causes", and talked to their MD's who all said they were killed by the vax, yet were all fired for telling the truth.