


Funding better COVID propaganda: The Mercury Project - Part 1
The Mercury Project has garnered over US$30 million to find out why people don't want COVID jabs, and how to persuade them to change their minds.

Question: If you were going to plough over US$30 million into funding research on why people are rejecting COVID-19 injections, would you name your research project after the Roman god of financial gain, commerce, trickery, and thieves, not to mention the guide of souls to the underworld? Welcome to the Mercury Project.
According to the promotional spiel from the Social Science Research Foundation, the nonprofit organisation which spawned the project,
“The Mercury Project is a global consortium of researchers dedicated to combating the impacts of mis- and disinformation on public health and to finding interventions that support the spread and uptake of accurate health information.”
Aw, that sounds nice, doesn’t it? I sure wouldn’t want to be exposed to mis- and disinformation on something as vitally important as public health; I bet you wouldn’t either.
Let’s keep reading.
“The Mercury Project, which alludes to the ancient Roman god Mercury of messages and communication [my note: funny how they left out the bit about financial gain, commerce, trickery, theft and guiding souls to the underworld], will fund researchers to discover new, evidence-based, data-driven tools, methods, and interventions to counter mis- and disinformation and to support the spread and uptake of accurate health information. These solutions will be an essential resource for social media and technology companies and for global policymakers as they build an information ecosystem that supports the sharing of accurate and effective health information.”
Right. So the nonprofit Social Science Research Council is going to be channelling tax-deductible donations into research to develop strategies which will then be used by for-profit Big Tech companies and by both elected and non-elected policymakers, to make sure that populations are exposed to health information that is deemed to be “accurate” (by whom, they don’t say, but I imagine you can guess) and “effective” (at what, they also don’t say, but you might like to have a stab at that, too).
Did anything in particular prompt this intense interest in mis- and dis-information? Let’s keep reading, shall we?
“The Mercury Project will provide research grants over a three-year period to researchers and organizations for the purpose of:
a) estimating the causal impacts of mis- and disinformation on online and offline outcomes in the context of the Covid-19 pandemic, including health, economic, and/or social outcomes, differential impacts across socio-demographic groups, and quantifying the global costs of those impacts;
b) estimating the causal impacts of online or offline interventions in the United States, Africa, Asia, and Latin America and the Caribbean to increase uptake of Covid-19 vaccines and other recommended public health measures by countering mis- and disinformation, including interventions that target the producers or the consumers of mis- and disinformation, or that increase confidence in reliable information.The Mercury Project will also provide a suite of research sharing and policy development activities for grantees and other invited organizations to enable more effective policy and regulatory responses to current and future public health emergencies. The work of the consortium will provide a foundation for data-driven policy and regulatory interventions enabling the creation of a healthier information environment.”
Ah, now we’re getting there. They want to find out why many people in sixteen low and middle-income countries (Bolivia, Brazil, Côte D’Ivoire, Kenya, Malawi, Ghana, Nigeria, Rwanda, Senegal, Sierra Leone, South Africa, Tanzania, Zimbabwe, India, Mexico and Haiti), as well as a substantial minority in the United States, rejected COVID-19 jabs.
They’re pretty sure it has something to do with wrongthink that has been disseminated online, so they’re going to experiment with a variety of messaging techniques to see which ones are the most successful at convincing people to believe what they want them to believe.
They’re also going to seek out better ways of shutting down voices that contradict their messaging, and help Big Tech out by developing better algorithms for suppressing content that doesn’t have the official stamp of approval, so that when the next big scary virus is released breaks out, the tax cattle will only be exposed to the kind of health information that they agree with.
Now, since the Social Science Research Council is a nonprofit, and we all know that such organisations are entirely benevolent, we can rest assured that the people running the Mercury Project are very well-intentioned. I'm sure glad about that, because if they weren't, they could be trampling all over fundamental human rights such as freedom of speech, not to mention aggressively censoring dissenting scientists and health practitioners who might have valuable information that the public has a right to know, for reasons that have nothing to do with our health and well-being.
Do you detect a note of sarcasm, dear reader? Good. You're paying attention.
Before we dig further into who and what is behind the Mercury Project, let's take a look at how the seventeen countries the project is targeting have done in terms of some of the key concerns that supposedly instigated the project: uptake of COVID-19 injections, deaths attributed to COVID-19, and excess mortality.
First, total doses of COVID-19 injections administered per 100 people in the countries that the Mercury Project is studying, with an aggregate of high income countries thrown in for comparison:
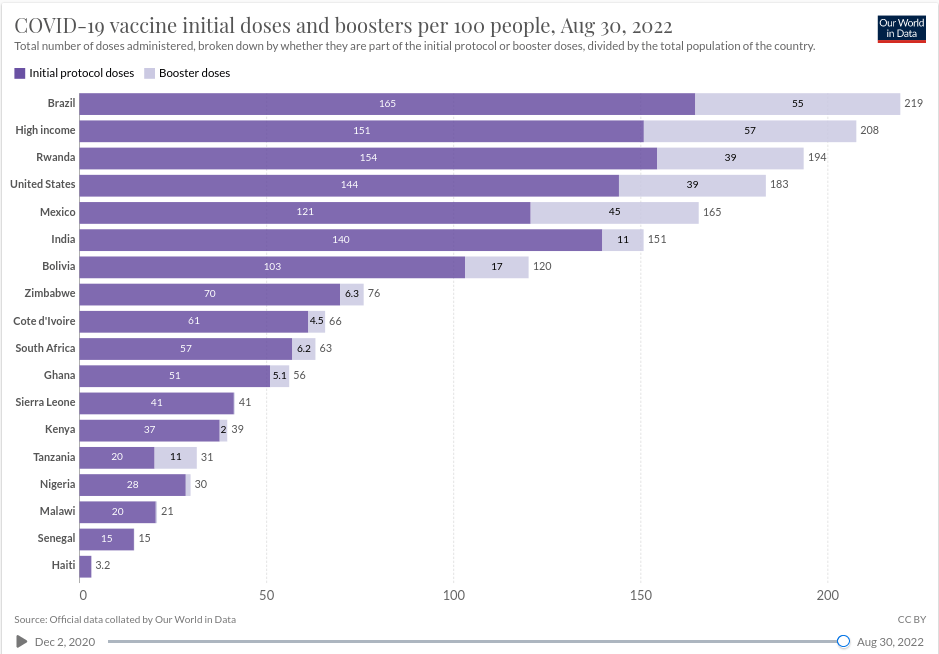
Note that Brazil, Rwanda and the US have had uptake rates that are comparable to the aggregate of high income countries, which raises the question, ‘Why target these countries for study?’ Are there, just possibly, sub-populations within these countries (say, ethnic minorities or partisans of a particular political persuasion, perhaps?) who have been particularly resistant to pro-injection messaging?
Now let’s look at deaths attributed to COVID-19, acknowledging that both countries and jurisdictions within them have taken varying approaches to categorising such deaths, which makes comparisons fraught with hazards:
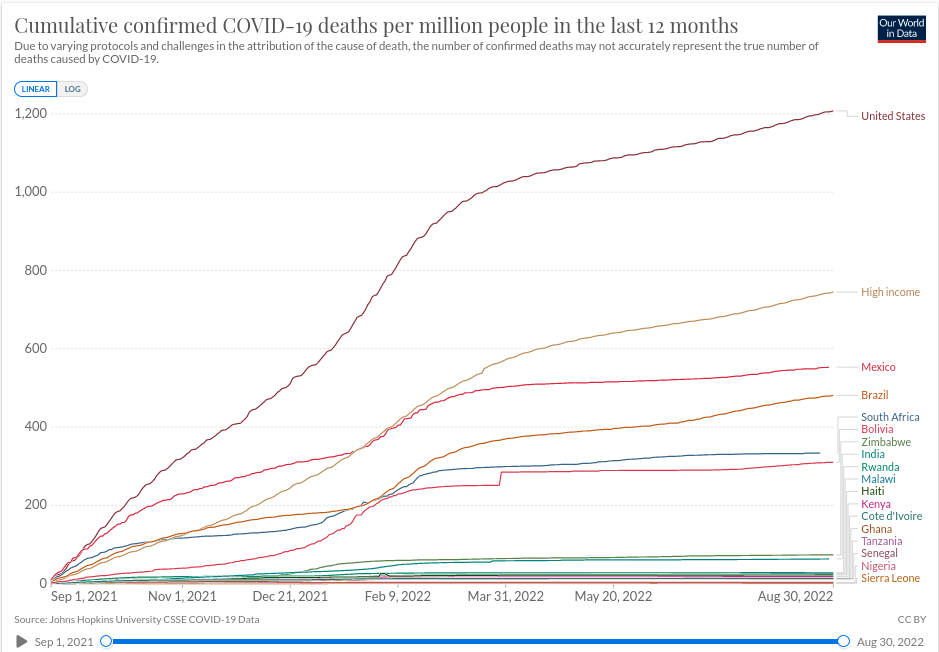
Notice how the countries with the lowest uptake of COVID-19 injections – Haiti, Senegal, Malawi, Nigeria, Tanzania, Kenya, Sierra Leone, Ghana – have the lowest death counts from the disease, while those with the highest uptakes – Brazil, the US and Mexico, along with high-income countries – have the highest death counts.
Rwanda is an interesting outlier, with high injection rates but a low COVID-attributed death rate. I have not dug into Rwanda’s injection campaign except to ascertain that they are using a mixture of Western, Chinese and Russian products (Moderna, Pfizer-BioNTech, AstraZeneca, Johnson & Johnson, Sinopharm and Sputnik V); if you, dear reader, can offer insight into the Rwandan situation, please leave a comment below.
While the inconsistencies in criteria for attributing deaths to COVID-19 can produce misleading comparisons, total deaths are not open to misinterpretation: dead is dead, after all. Hence, excess mortality – a measure of how many more people have actually died than were expected to die, based on past death counts and current demographic data – can be used to gain insight into the impact of the entire COVID-19 package: the SARS-CoV-2 virus itself; the containment measures imposed by governments, which were especially deadly to the poorest of the poor who rapidly starve if they are prevented from going out to work; the medical treatments applied to those with COVID-19; and the injections that were supposed to protect people against the disease.
Of course, the contribution made by each of these factors can’t be teased out of excess mortality data, but at minimum, we would expect that if COVID-19 injections did what they were supposed to do, we should see lower excess mortality in the countries with the highest rates of injection.
Let’s take a look:
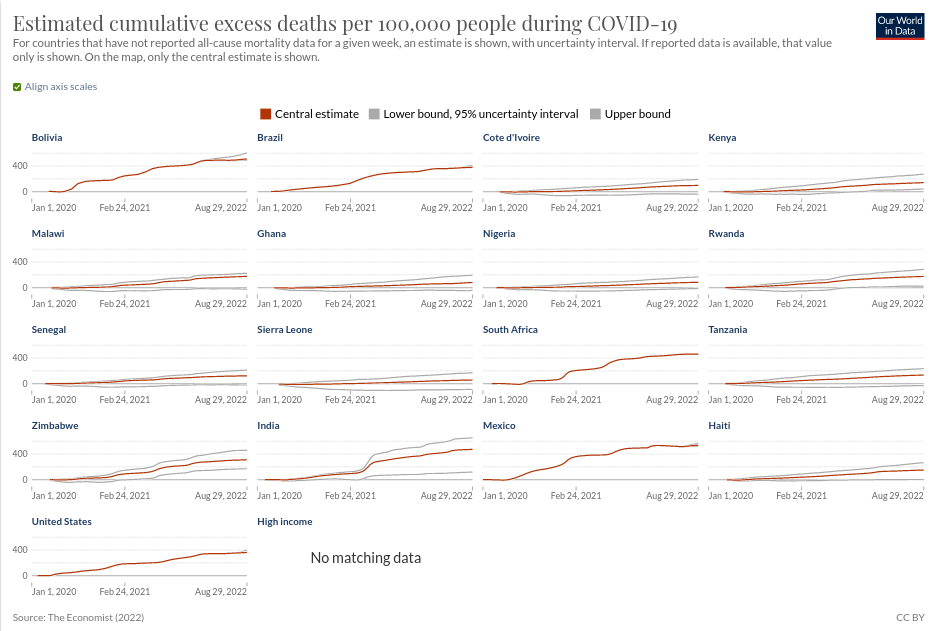
Again, low-injection-rate Haiti, Senegal, Malawi, Nigeria, Tanzania, Kenya, Sierra Leone and Ghana all have lower excess mortality than high-injection-rate Brazil, the US and Mexico, with highly-jabbed Rwanda once again an outlier.
Given that, out of the seventeen countries being targeted by the Mercury Project, those with the lowest uptake of COVID-19 injections have done the best with respect to both COVID-19 deaths and excess mortality, the claim that the project was motivated by the benevolent desire to protect the public against the damaging effects of health mis- and disinformation is starting to ring hollow.
Whatever forms of unsanctioned information the people in countries which largely rejected the injections were exposed to, it doesn’t seem to have harmed their health – at least, if we can all agree that not being dead might have some utility as an indicator of health.
So what did motivate the Social Science Research Council (SSRC) to commission the Mercury Project? In an interview conducted for Philanthropy Now, SSRC president, Anna Harvey, fretted that “public health experts have been taken aback by the ferocity and virulence of the misinformation the [COVID-19] pandemic has unleashed”.
Harvey went on,
“Last year, we thought that by this time this year, everybody would be vaccinated—except those who have medical conditions that prevent them from being vaccinated [my note: I haven’t encountered a single person who has been able to obtain a medical exemption, even when they have a pre-existing medical condition that increases their risk of adverse reactions or have had a previous adverse reaction to the COVID-19 jabs] —and we would be distributing vaccines around the world. But we’re just so far from that goal… It took a while for the realization to dawn that we were up against something that we hadn’t really seen before.”
The Global “Infodemic” Poses Serious Health Risks. Can Philanthropy Help Find a Cure?
“Something that we hadn’t really seen before” – you mean, people objecting to being misled, cajoled, bribed, coerced or outright forced into receiving an inadequately-tested, rushed-to-market, liability-free experimental injection which neither prevents infection with, nor transmission of, a virus with a median infection fatality rate of 0.27%? Yeah, I guess we haven’t seen that before.
But it’s not just the widespread and growing resistance to COVID-19 injections that’s got the SSRC’s knickers in a twist. They’re now seeing “pushback against the COVID vaccine feed into formerly fringe areas of vaccine resistance.”
According to Harvey,
“We’re seeing legislation in some states to roll back requirements for childhood vaccines. These are things we thought were settled public health initiatives.”
The Global “Infodemic” Poses Serious Health Risks. Can Philanthropy Help Find a Cure
Yes, as I’ve reported in several previous articles including Are doctors the new antivaxxers?, Why you need to stop saying “I’m not an antivaxxer, but…” and Backlash: How the vaccine pushers turned true believers into vaccine sceptics – Part 1, once people have woken up to the fact that public health authorities have been blatantly lying to them about the “safe and effective” COVID-19 shots, many of them start to wonder if they’ve been just as mendacious about the rest of the vaccination schedule. Go figure.
And Ms Harvey and co are not going to sit back and allow people to make their own decisions when it comes to which vaccines they will and won’t accept, for themselves and their children. You see, you plebs aren’t capable of differentiating between “health mis- and disinformation” and “accurate and effective” health information, so you need to be properly informed by public health authorities – you know, the ones that told you that the COVID-19 injections were safe and effective.

As an example of how important it is that the right people be in charge of disseminating “accurate and effective” health information, Connie Matthiessen, author of the Inside Philanthropy article, opened by citing a particularly harrrowing example of health misinformation: the promotion of the use of “horse deworming medicine as a cure for COVID”.
Yes, she really, truly wrote that. She really did describe ivermectin – a medicine which won its developers the 2015 Nobel Prize for Physiology or Medicine, for its role in conquering some of the world’s most devastating tropical diseases, and which also possesses broad-spectrum antiviral activity against a plethora of viruses including Zika, dengue, yellow fever, West Nile, Hendra, Human immunodeficiency virus type 1… and SARS-CoV-2 – as a “horse dewormer”.
Pot, meet kettle.
By the way, here’s how that “horse dewormer” stacks up as a “cure for COVID”:

But I guess Matthieson would prefer the treatments promoted by those purveyors of “accurate and effective” health information such as molnupiravir:
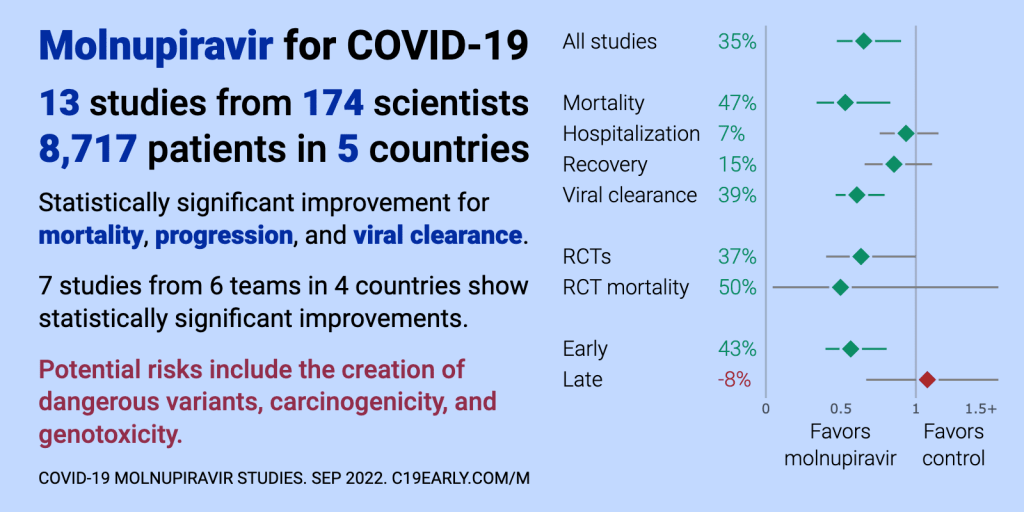
… or paxlovid:

… or remdesivir:

I’ll bet you’re glad that purveyors of journalistic truthiness like Connie Matthiessen are on the side of the people who have tasked themselves with responding to “calls from the World Health Organization, the U.S. Office of the Surgeon General, and the Aspen Institute’s Commission on Information Disorder” – yes, “information disorder” is a thing; who knew? – to combat the “infodemic” – also a thing which, according to the World Health Organization (WHO), “leads to mistrust in health authorities and undermines the public health response”.
But wait, it gets even better. Matthiessen goes on to cite a fact sheet co-written by the WHO and the Pan American Health Organization which, in the midst of six pages of blather about people believing stuff they read on the interwebs instead of “trusted sources” like themselves (helpfully illustrated with a dodgy clip-art graphic depicting… something-or-other), states:
“Inaccurate and false information has been circulating about all aspects of the disease: how the virus originated, its cause, its treatment, and its mechanism of spread. All this makes the pandemic much more severe, harming more people and jeopardizing the reach and sustainability of the global health system.”
Understanding the infodemic and misinformation in the fight against COVID-19
Damn straight there was “inaccurate and false information” circulating about SARS-CoV-2 and COVID-19 at the time this “fact sheet” was published, in 2020, and the WHO was one of the most flagrant purveyors of it.
The WHO:
Parroted Chinese officials’ claims that there was no evidence of human-to-human transmission of SARS-CoV-2, at a time when American journalists who had evidence that the Chinese government was instituting a cover-up, were being expelled from the country. The delay in acknowledging human-to-human transmission resulted in rapid global spread of the virus along with inadequate preparations for its inevitable arrival, thanks to the WHO enabling Chinese Communist Party deceit.
Effusively praised China’s draconian response to the emergence of SARS-CoV-2, which defied all previous guidance on the management of respiratory pandemics, including WHO’s own International Health Regulations, and encouraged other countries to follow China’s lead. Aggressive containment measures have been comprehensively demonstrated to have no discernible effect on reducing serious illness or death in any jurisdiction that enacted them.
Dismissed the possibility that SARS-CoV-2 could have escaped from the Wuhan Institute of Virology after conducting a 12-day fact-finding mission to China, over a year after the outbreak began. Among the 17 mission members was Peter Daszak, who heads EcoHealth Alliance, the nonprofit which, since 2008, has received almost US$42 million in grant funding from the US Department of Defense to conduct research on “countering biological weapons”, much of it funnelled to – you guessed it – the Wuhan Institute of Virology. Mission leader Peter Ben Embarek later disclosed that the WHO team was subjected to enormous pressure to not even consider the lab leak theory by Chinese officials, a small army of whom accompanied them at all times. The Chinese only agreed to discuss the possibility of a lab leak 48 hours before the conclusion of the mission, "on the condition we didn’t recommend any specific studies to further that hypothesis."
Designed and ran a multi-centre randomised controlled study (the Solidarity trial) on hydroxychloroquine for the treatment of COVID-19, which prescribed a dose of the drug that is well known to be potentially toxic and even life-threatening. They persisted with this dosage regime even after the Indian Council of Medical Research wrote to WHO to express concern that the hydroxychloroquine doses being used in the Solidarity trial were 4 times higher than the doses being used in India. After an excess of deaths was, rather unsurprisingly, observed in patients assigned a toxic dose of hydroxychloroquine, WHO halted the trial and recommended against the use of the drug for treatment of COVID-19.
Denied until well into 2021 that SARS-CoV-2 was spread primarily by airborne transmission rather than respiratory droplets. This seemingly arcane distinction has tremendous implications for public health policy – namely, any facial masks short of fit-tested N95s worn by everyone, all the time, are useless; maintaining some random number of metres of distance from other people is beyond ridiculous, because airborne particles can travel many metres in still air; those stupid plexiglass barriers actually increase the risk of viral transmission by interfering with air flow, which is the most important factor in mitigating airborne transmission; and all that hand sanitising and surface cleaning is almost completely pointless, as there’s a less than 1 in 10 000 chance of getting infected by touching a contaminated surface.
Given this truly impressive track record of disseminating health mis- and disinformation, I wonder whether the good folk at the Social Science Research Council should cancel all their grants for such projects as developing “counter-messaging” to “emerging health misinformation” on “English-speaking Twitter”; snooping on the Whats App networks of Sierra Leonians to find out if they will persuade each other to get a COVID jab; and brainwashing Indian high school students – I mean, “inoculating [them] against misinformation”; and study the WHO instead. Why not learn from the masters?
But of course, the SSRC’s grantees won’t be doing that. Instead, they’ll be focusing their tender ministrations on those poor benighted black and brown people in Africa, Asia and Latin America, as well as the knuckle-dragging US anti-vaxxers who watch “right wing media figures like Fox News host Tucker Carlson” and fall for disinformation from “Russian sources” (which is apparently purveyed primarily via seriously lame cartoons).
And they’ll have plenty of lovely grant money to lavish on their worthy projects – the initial US$7.2 million in direct research funds was recently topped up with an additional US$20 million from the National Science Foundation (a supposedly “independent” agency of the United States government) which has formed a partnership with the Mercury Project.
Why spend all that dough to find out why people don’t want to take injections that don’t protect them from getting a disease that they have a vanishingly small risk of dying from? Don’t forget, the Mercury Project is intended to develop “more effective policy and regulatory responses to current and future public health emergencies”. They’re investing money now with the aim of reaping the rewards next time around.
By now, I'll bet you're on the edge of your seat to find out just who are the organisations funding the Mercury Project, and what are their aims. Don't worry, we'll get to that... in Part 2. Stay tuned!
Great work Robyn, this is an important topic that needs some light. Unfortunately, I think the ultimate form of coercion is digital currency. Once the ability to conduct financial transactions is stopped for various non-compliance , then things will get very interesting indeed.
Great article Robyn. Speaking of propaganda, this came out in the states today (see below). It illuminates the massive free speech suppression campaign going in the U.S. Completely illegal, but when has that stopped the government before.
https://www.zerohedge.com/political/twitter-facebook-regularly-coordinated-biden-admin-censor-users