


An open letter to Australian politicians on COVID-19 vaccine mandates for healthcare workers

Following is a letter which I am sending to every Queensland and Federal member of parliament and senator in response to the Chief Health Officer’s direction that all heathcare providers must be “fully vaccinated” against COVID-19 by 15 December 2021. I encourage readers to present this open letter to their own local member and senator, and give full permission to reproduce it in whole or in part.
I encourage all Queensland healthcare practitioners, whether medical, allied health or complementary, who are opposed to the CHO direction mandating COVID-19 vaccination, to join the Queensland Health Practitioners Association and contribute to our legal fighting fund. Members of the public who wish to support practitioners’ right to choose whether or not to receive a COVID-19 vaccine can contribute via MyCause.
You can download the letter as a PDF file here.
Dear Sir/Madam
As I am sure you are aware, the Chief Health Officer of Queensland has issued a direction1 ordering that by 15 December 2021, all persons who work in a healthcare setting must have received two doses of a COVID-19 vaccine, with the maximum penalty for noncompliance being 100 penalty units (i.e. $13,785) or 6 months imprisonment.
I am a sole practitioner in a home-based Lifestyle Medicine clinic. Unless I comply with this directive, I will no longer be able to see clients in person. Whilst hairdressers, beauty therapists, and massage therapists (including those who provide “non therapeutic” massage) are not subject to a vaccine mandate2 despite working in extremely close proximity to their clients, the Chief Health Officer of Queensland judges that clients sitting opposite me in a well-ventilated room would be at an unacceptable risk of infection unless I am “fully vaccinated”.
Australia’s COVID-19 policies are scientifically unsound
I have an Honours degree in Public Health, a qualification which taught me the history and mission of the public health movement, as well as how to read, understand and critique scientific literature. The former outcome of my academic training – understanding the mission of public health – alerted me to the fact that the Federal and State policy responses to the emergence of SARS-CoV-2 are uniformly disastrous from a public health standpoint. Not only have these policy responses completely abandoned the evidence-based protocols laid out in the Australian Health Management Plan for Pandemic Influenza3, they violate the foundational principle laid down by D.A. Henderson, the man who designed the strategy which resulted in the eradication of smallpox:
“Experience has shown that communities faced with epidemics or other adverse events respond best and with the least anxiety when the normal social functioning of the community is least disrupted. Strong political and public health leadership to provide reassurance and to ensure that needed medical care services are provided are critical elements. If either is seen to be less than optimal, a manageable epidemic could move toward catastrophe.”4
Disease Mitigation Measures in the Control of Pandemic Influenza
State and Federal policies aiming to “stop the spread” of SARS-CoV-2 (a fool’s errand with a highly contagious but low virulence airborne virus) have indeed been catastrophically disruptive to normal social functioning, have stoked rather than allayed public anxiety, and have resulted in the denial of needed medical care to the public by prohibiting access to safe and inexpensive early effective treatment for COVID-195, 6, which has been repeatedly shown to reduce the risk of hospitalisation and death by at least 85%, even in high-risk elderly patients7, 8, 9.
The latter outcome of my academic training – ability to read and understand medical and scientific literature – has alerted me to two pivotal facts:
1. The risk of COVID-19 vaccines exceeds the benefits, for individuals in all age groups
The risk:benefit ratio of receiving any of the products described as “COVID-19 vaccines” currently available in Australia is extremely unfavourable to me personally; that is, I am far more likely to experience a serious adverse event than I am to be made seriously ill from SARS-CoV-2 infection. According to an exhaustive analysis by Kostoff et al10,
“A novel best-case scenario cost-benefit analysis showed very conservatively that there are five times the number of deaths attributable to each inoculation vs those attributable to COVID-19 in the most vulnerable 65+ demographic. The risk of death from COVID-19 decreases drastically as age decreases, and the longer-term effects of the inoculations on lower age groups will increase their risk-benefit ratio, perhaps substantially.”
Why are we vaccinating children against COVID-19?
In other words, as a healthy, normal-weight 50 year old with no comorbidities, my risk of dying as a result of receiving any of the currently-available COVID-19 vaccines exceeds my risk of dying of COVID-19 itself by substantially more than five times.
According to the University of Oxford’s QCovid Calculator11, my personal risk of a COVID-19-associated death if unvaccinated is 1 in 111,111, based on data collected in the second and third pandemic waves in England. Using US and Australian data, MyCOVIDOdds12 calculates my risk of dying if infected with the Delta variant of SARS-CoV-2 at 1 in 50,250 if I receive no treatment, or 1 in 334,983 with evidence-based early treatment.
Given the vanishingly small likelihood that I would become seriously ill or die as a result of SARS-CoV-2 infection, even a low likelihood of injury by COVID-19 vaccines would be quite simply unacceptable to me.
However, the risk of injury is not low. All pharmacovigilance systems including DAEN in Australia, VAERS in the US, the Yellow Card system in the UK, EudraVigilance in the EU and the WHO’s VigiBase are raising safety signals to a degree unprecedented in their history. I must stress that the purpose of pharmacovigilance systems is not to prove causation but to detect safety signals which must then be thoroughly investigated through both examination of patient clinical records and pathology (including autopsy) specimens, and data analytics. One way of detecting such signals is to compare adverse event reports between different vaccine products.
The comparison between adverse event and death reports to DAEN associated with COVID-19 vs influenza vaccines is striking:

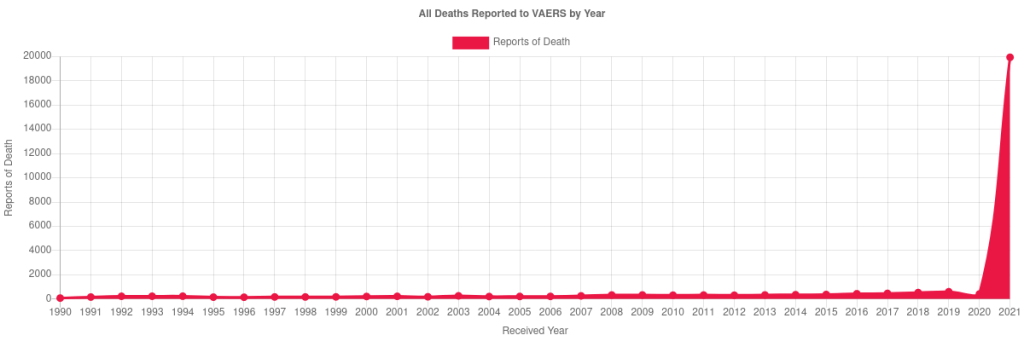
The number of deaths reported to VAERS in association with receipt of a COVID-19 vaccine is clearly wildly in excess of any other vaccine13:
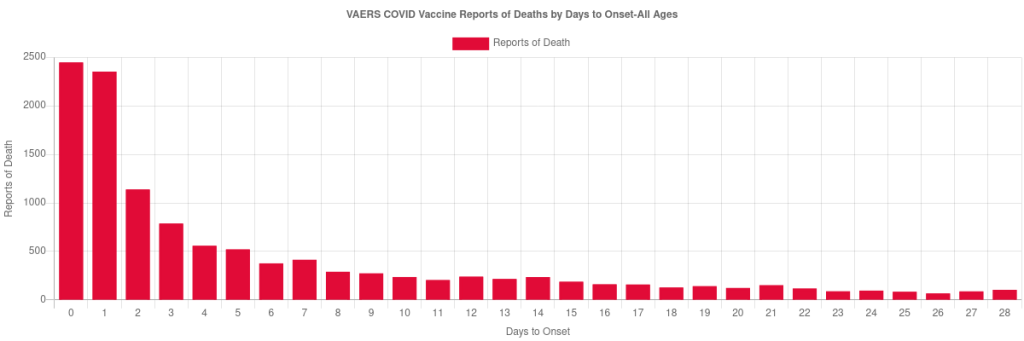
Furthermore, there is a strong temporal relationship between vaccination and death. If there were no causal relationship between receipt of the vaccine and death, death reports would be evenly distributed over the days following vaccination, but in fact it is obvious that deaths cluster in the few days following vaccination before gradually tapering off14:
The recent revelation, forced by a Freedom of Information request, that Pfizer received 42,086 case reports of serious adverse reactions to its COVID-19 vaccine – including 1223 deaths – in just the first 90 days of the worldwide rollout, with thousands more submissions omitted from the report15, reinforces my view (which is backed by international experts in drug safety including Dr Tess Lawrie of the Evidence-based Medicine Consultancy16 and vaccinologist Dr Geert Vanden Bossche17) that these products are unacceptably unsafe.
For comparison, the 1976 swine flu vaccination campaign was halted after only around 30 vaccine-associated deaths were reported18.
2. COVID-19 vaccines do not stop infection with or transmission of SARS-CoV-2 and hence cannot end the COVID-19 pandemic
Despite the rhetoric of both politicians and public health officials in Australia, the products described as COVID-19 vaccines do not prevent infection with, nor transmission of, SARS-CoV-2; they merely reduce the symptoms of infection. The evidence that I summarise for you below clearly demonstrates that far from protecting my clients, if I did accept a COVID-19 vaccine and subsequently became infected with SARS-CoV-2, I would present a greater hazard to them than if I developed an infection whilst unvaccinated, since I would be less likely to have any symptoms to warn me that I was ill and should self-isolate, at the point where I was at peak viral load and therefore maximal risk for infecting others.
State and Federal policies on vaccination have been informed by modelling performed by the Doherty Institute. However, this modelling rests on outdated assumptions that have been disproven by more recent and thorough research. Furthermore, the Doherty Institute has misrepresented its data sources for key calculations.
For example, the following table from Doherty’s August modelling update19 estimated that COVID-19 vaccination would reduce the risk of household transmission of SARS-CoV-2 in a fully vaccinated person with a breakthrough infection of the Delta variant by 65%:
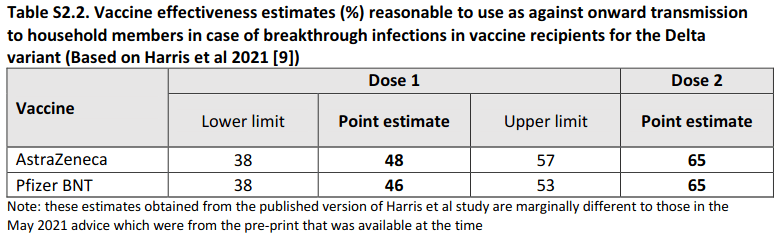
However, the “study” referenced in the table caption is actually a letter to the editor of the New England Journal of Medicine (i.e. not subject to normal peer-review processes)20 which drew on a dataset of COVID-19 cases identified in England between 4th January and 28th February 2021, when the Alpha variant of SARS-CoV-2 accounted for the overwhelming majority of UK COVID-19 cases. In fact, the Delta variant was not detected in the UK until mid-April 202121. In addition, the authors of this letter stated that “most of the vaccinated index patients in our data set (93%) had received only the first dose of vaccine.” From where, then, does Doherty derive its point estimate for vaccine effectiveness after dose 2? Certainly not from the article that it cites as the source of its calculations!
A peer-reviewed study examining UK contact tracing data, published in The Lancet on October 29, 202122 found that a person who had received a COVID-19 vaccination but developed a breakthrough infection was not less likely to transmit the virus to a household member than an unvaccinated individual; in fact rates of transmission were virtually identical:
“SAR [secondary attack rate] among household contacts exposed to fully vaccinated index cases was similar to household contacts exposed to unvaccinated index cases (25% [95% CI 15–35] for vaccinated vs 23% [15–31] for unvaccinated).”
Community transmission and viral load kinetics of the SARS-CoV-2 delta (B.1.617.2) variant in vaccinated and unvaccinated individuals in the UK: a prospective, longitudinal, cohort study
The difference in risk of infection between vaccinated and unvaccinated household contacts of an individual with a Delta strain infection did not reach statistical significance. Overall, vaccine effectiveness was estimated to be just 34%, well below the 50% threshold set by the FDA for approval of a vaccine, and substantially below the Doherty Institute’s projections for the effectiveness of the Pfizer and AstraZeneca vaccines against the Delta strain (79% and 60% respectively; see Table S2.1 below). These projections have informed State and Federal government policies, but were based on a study23 of cases identified in Scotland between April 1, 2021 (when the Alpha variant was still dominant in the UK) and June 6, 2021 (when the Delta variant accounted for 80% of cases in which genetic sequencing was performed; it was not until late May that Delta cases outstripped Alpha in the UK)24:
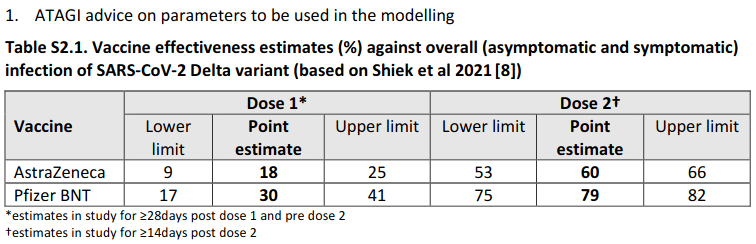
Astonishingly, the Doherty Institute’s latest update to Federal Cabinet, dated 5 November 202125, assumes vaccine effectiveness against infection and onwards transmission of 79% for the AstraZeneca product and 93% for the Pfizer product, in direct contradiction to real-world evidence.
Real-world evidence that COVID-19 vaccines do not protect other people
1) A pre-print study of US prisoners26 found no difference in cycle threshold values (an indicator of viral load) between breakthrough infections and infections in unvaccinated individuals; no difference in the length of time that fully vaccinated vs unvaccinated participants tested positive on RT-PCR for SARS-CoV-2, and no difference in the duration of viral culture positivity (an indicator that infectious virus is present, as opposed to noninfectious viral particles that linger after infection has resolved) between fully vaccinated vs unvaccinated participants. In other words, vaccinated individuals were equally as likely to infect others as unvaccinated individuals.
2) Likewise, a pre-print study conducted in two demographically-distinct sites in California during the Delta surge27 found no significant difference in cycle threshold values between vaccinated and unvaccinated, asymptomatic and symptomatic groups infected with the Delta strain of SARS-CoV-2. The authors of the study concluded that:
“A substantial proportion of asymptomatic, fully vaccinated individuals in our study had low Ct-values, indicative of high viral loads. Given that low Ct-values are indicative of high levels of virus, culture positivity, and increased transmission [11], our detection of low Ct-values in asymptomatic, fully vaccinated individuals is consistent with the potential for transmission from breakthrough infections prior to any emergence of symptoms.”
No Significant Difference in Viral Load Between Vaccinated and Unvaccinated, Asymptomatic and Symptomatic Groups When Infected with SARS-CoV-2 Delta Variant
In plain language, the vaccinated are at high risk of infecting other people, whether they display symptoms of COVID-19 or not.
3) A pre-print study conducted by public health officials from the US state of Wisconsin28 reached similar conclusions: fully vaccinated individuals were slightly more likely to have low Ct values (indicating higher viral load) than unvaccinated individuals (68% vs 63%), 95% of low-Ct samples from fully vaccinated individuals contained infectious SARS-CoV-2 vs 88% of low-Ct samples from unvaccinated individuals; and there were no difference in infectious virus titer between groups. Furthermore, “low Ct values were detected in vaccinated people regardless of symptoms at the time of testing”, and “infectious virus was detected in the sole specimen tested from an asymptomatic fully vaccinated individual”. Once again, this study found that vaccinated individuals were at least as likely, if not more so, to infect others as unvaccinated people and that they could do so whilst remaining asymptomatic themselves.
4) A pre-print study using contact tracing data from England29 found that the Pfizer vaccine reduced onward transmission of the virus by 50% at 2 weeks after the second dose, and only 24% at 12 weeks after the second dose. Performance of the AstraZeneca vaccine was even worse: it reduced onward transmission by only 24% at 2 weeks after the second dose, and a mere 2% at 12 weeks after the second dose. In other words, neither product offered effective protection against onward transmission of the Delta even at the point where they are considered to be at the peak of their protective effect.
5) On the other side of the transmission chain, a Swedish study30 found that the vaccine effectiveness of the Pfizer product against becoming infected waned progressively from 92% at days 15-30 after receiving the second dose, to 47% at days 121-180, and from day 211 onwards no effectiveness was detected. Vaccine effectiveness waned slightly slower for the Moderna product, estimated at 59% from day 181 onwards. The AstraZeneca product reached negative efficacy (i.e. caused a 19% increased risk of infection) from day 121.
Selfish vaccines
To put it bluntly, these are selfish vaccines. The only benefit they offer is to temporarily reduce the risk of developing symptoms of COVID-19 in the person who has received them, but this comes at the cost of the vaccinated person becoming a potential “Typhoid Mary”. That is, the vaccinated person may become infected but remain asymptomatic, potentially shedding infectious virus onto both vaccinated and unvaccinated individuals, including vulnerable people at high risk of serious COVID-19 illness. By contrast, an unvaccinated person who becomes infected is more likely to develop symptoms of illness which alert them to get tested and to self-isolate, thereby protecting others. And by definition, an unvaccinated person who is not infected is no risk to anyone.
Despite the constant rhetoric that COVID-19 vaccines are our only way out of the pandemic, no country which has achieved high vaccination rates has succeeded in bringing SARS-CoV-2 under control. In fact, a study of 68 countries and 2947 counties in the United States31 found that not only did high vaccination rates fail to bring down case counts, but in fact “countries with higher percentage of population fully vaccinated have higher COVID-19 cases per 1 million people”. Within the US,
“Of the top 5 counties that have the highest percentage of population fully vaccinated (99.9–84.3%), the US Centers for Disease Control and Prevention (CDC) identifies 4 of them as “High” Transmission counties. Chattahoochee (Georgia), McKinley (New Mexico), and Arecibo (Puerto Rico) counties have above 90% of their population fully vaccinated with all three being classified as “High” transmission. Conversely, of the 57 counties that have been classified as “low” transmission counties by the CDC, 26.3% (15) have percentage of population fully vaccinated below 20%.”
Increases in COVID-19 are unrelated to levels of vaccination across 68 countries and 2947 counties in the United States
Scientists from highly-vaccinated countries are sounding the alarm that vaccinated individuals are driving transmission and warning that scapegoating and stigmatisation of unvaccinated individuals is scientifically wrong and sociopolitically extremely dangerous; see for example Günter Kampf’s letter to The Lancet32 which summarises some of the most recent studies demonstrating the role that vaccinated individuals play in transmitting SARS-CoV-2 to others and concludes that:
“There is increasing evidence that vaccinated individuals continue to have a relevant role in transmission… It is therefore wrong and dangerous to speak of a pandemic of the unvaccinated. Historically, both the USA and Germany have engendered negative experiences by stigmatising parts of the population for their skin colour or religion. I call on high-level officials and scientists to stop the inappropriate stigmatisation of unvaccinated people, who include our patients, colleagues, and other fellow citizens, and to put extra effort into bringing society together.”
COVID-19: stigmatising the unvaccinated is not justified
As an elected representative, you should be gravely concerned that both State and Federal governments are acting on advice derived from modelling from the Doherty Institute which misrepresents its data sources and is completely divorced from the real-world evidence presented by the scientific literature. Furthermore, this poor advice is being leveraged by politicians and health bureaucrats to infringe on the liberties, livelihood and health of your constituents and is feeding increasingly unhinged political rhetoric that is creating deep and potentially dangerous social divisions between vaccinated and unvaccinated Australians.
It should at least pique your curiosity that a substantial proportion of healthcare workers – including doctors, nurses, paramedics, allied and complementary practitioners – do not wish to receive a COVID-19 vaccine. Remember that these are people who know how to read scientific literature and are observing first-hand the alarming impact of COVID-19 vaccines on their clients and patients. Ask yourself why so many such people would be willing to give up careers for which they have spent many years training and developing their skills, in order not to have these products forced upon them.
And you should also note that vaccination mandates directly contravene the informed consent requirements of the Australian Immunisation Handbook33, which specify that “for consent to be legally valid… it must be given voluntarily in the absence of undue pressure, coercion or manipulation.” It goes without saying that the Queensland CHO directive, which denies health professionals the right to earn a livelihood if they do not accept a COVID-19 vaccine, constitutes coercion, and therefore violates the principle of informed consent and renders any consent extracted through such coercion, legally invalid. As I have clearly laid out for you, there is no scientific justification for this violation since COVID-19 vaccines offer no benefit except to the person who receives them, and then only symptomatically and temporarily.
As I have taken the time to explain the reasons for my objection to de facto compulsory vaccination, and to document them with reference to scientific literature, I expect a thoughtful and specific response from you. A pro forma reply is not acceptable and will result in repeated emails, letters and phone calls to your office until I receive a response which specifically answers my key question: Why am I being mandated to receive a COVID-19 vaccine that is not safe and does not prevent me from infecting my clients with SARS-CoV-2?
Yours sincerely
Robyn Chuter
BHSc(Hons), ND, GradDipCouns, Fellow of the Australasian Society of Lifestyle Medicine
Thanks for laying it out so succinctly. It seems that the 'vaccines ' scramble peoples brains to such an extent that they can't think logically any more. Seriously though, people generally do not want to admit their mistakes, and therefore, even with all the evidence stacking up in front of them, our 'leaders' don't want to dismantle all the crazy rules and mandates. That is the human condition, sorry to say.
Thanks Robyn for your truthful analysis. It’s a blessing to know that some people even though they are the minority are not fooled by the lies scandal and coverups coming from Government Health Authority.